
Laparoscopic Sigmoid Resection for Diverticulitis
Main Text
Table of Contents
Laparoscopic low anterior resection (LAR) is indicated for disease of the distal sigmoid or rectum that requires resection, most notably diverticulitis and colorectal cancer. Here, we perform an LAR for diverticular disease. In this procedure, we used four laparoscopic port sites. In the first step, we mobilized the splenic flexure and left colon to allow for a tension-free colorectal anastomosis low in the pelvis. Second, the mesorectum was dissected to mobilize the rectum down to the level of the pelvic floor. Third, the left colic and inferior mesenteric arteries were ligated, the colonic mesentery was transected with an energy device, and the distal resection margin was stapled intracorporeally. Fourth, the specimen was extracorporealized through the umbilical port site and the proximal transection was performed. Finally, an anvil was inserted, and the colon was placed back into the abdomen where a trans-anal, stapled end-to-side Baker anastomosis was performed and endoscopically tested for leaks.
Diverticulosis is a process by which colonic mucosa and submucosa herniate between muscular layers of the bowel wall to form false diverticula. Diverticulosis occurs in 60% of Americans aged greater than 60 years; it is thought to be associated with a low fiber, Western diet, obesity, and physical inactivity.1 Although diverticulosis can occur anywhere in the colon, it presents more commonly in the distal left colon and sigmoid. Diverticula can become obstructed with fecal matter, resulting in venous congestion, tissue ischemia, inflammation, infection, and, in severe cases, perforation, a process referred to as diverticulitis.2 Diverticulitis affects 10-25% of patients with diverticulosis, and represents a significant healthcare burden in the United States, accounting for 2.7 million outpatient visits and over 200,000 inpatient admissions each year.3 Diverticulitis presents with varying degrees of severity. Uncomplicated disease is limited to local inflammation and pain, whereas complicated diverticulitis is associated with perforation that can result in abscess, phlegmon, or purulent/feculent peritonitis that may require urgent surgical intervention. Long-term complications of diverticulitis include stricture and fistula formation to surrounding structures.
Treatment for diverticulitis depends on disease severity and acuity. Uncomplicated disease is initially treated with antibiotics, intravenous fluids, and bowel rest. Complicated disease may require surgical intervention. For perforated diverticulitis with abscess, percutaneous drainage may be indicated for source control. Purulent or feculent peritonitis may require urgent surgical intervention, usually with resection of the diseased colon, and either fecal diversion with end-colostomy (Hartmann’s procedure) or primary colorectal anastomosis if conditions permit.4 There are certain indications for colectomy on an elective basis for diverticulitis. Surgery is recommended for patients who are at high risk for infection, e.g. immunosuppressed transplant patients, patients with prior episodes of diverticulitis with abscess that required drainage, those with long-term complications such as fistula or stricture, and for patients who have had multiple recurrent episodes and would like to prevent future occurrences.5
In the present case, we perform an LAR for sigmoid diverticulitis in a 70-year-old patient who had three prior episodes of uncomplicated diverticulitis over the prior year. In the LAR procedure, the sigmoid and proximal rectum were excised and a colorectal anastomosis was performed. The procedure adequately resected the diseased portion of colon, effectively treating this condition.
The patient is a 70-year-old female presenting with recurrent, uncomplicated diverticulitis that was negatively impacting her quality of life. She had experienced 12-15 episodes over the prior decade, three of which occurred within the last 12 months, and she presented for elective resection. The prior episodes were treated with antibiotics. Her other medical history is notable for early stage breast cancer treated with lumpectomy. She had a surgical history notable for a salpingectomy and oophorectomy to treat an ectopic pregnancy over 30 years prior. She had an American Society of Anaesthesiologist score of 2 and her body mass index was 21. Preoperative evaluation included a colonoscopy that confirmed diverticulosis without evidence of malignancy.
The patient had an unremarkable physical exam. In the office, she was in no apparent distress with normal vital signs. She had a normal habitus. Her abdominal exam was significant for prior surgical scars, no evidence of hernias, and no tenderness to palpation.
The patient’s most recent episode of diverticulitis was 10 weeks prior to her elective surgery. At that time, she presented to the emergency department with abdominal pain and underwent a computed tomography (CT) scan of the abdomen and pelvis with oral and intravenous contrast, revealing evidence of sigmoid diverticulitis without perforation (Figure 1).
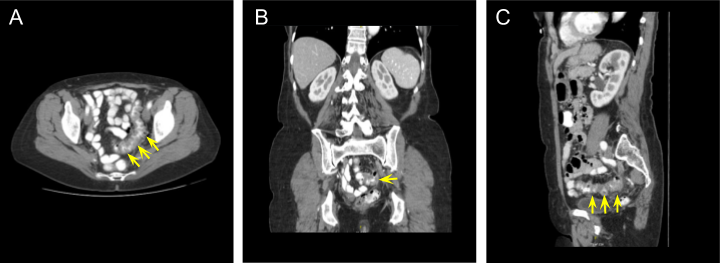
Figure 1. Abdominal and Pelvic CT Scan CT scan of the abdomen and pelvis with intravenous and oral contrast revealing evidence of uncomplicated sigmoid diverticulitis. The diseased tissue is shown in (A) axial, (B) coronal, and (C) sagittal views. Yellow arrows point to the diseased segment of colon.
Our understanding of the natural history of diverticulitis has recently come under scrutiny. It was previously thought that diverticulitis is a progressive condition in which recurrent disease is associated with more severe complications. This paradigm was the foundation for an aggressive surgical approach. However, more recent data suggested that complications are most likely to occur during the first episode, with decreased severity during subsequent episodes.6 In response to this information, a more conservative approach to treatment is currently practiced. Nevertheless, the risk of recurrence does increase with subsequent episodes. The risk of recurrence after a first episode of uncomplicated diverticulitis is approximately 20% at 10 years, increasing to greater than 50% after a second episode.7
The only potentially curative therapy for diverticulitis remains surgical resection of the diseased tissue. Nevertheless, elective colectomy is not essential, and the patient should discuss the risks and benefits of an operation with their surgeon. Other potential treatments, including dietary changes, probiotics, and certain pharmacologic agents are under investigation; however, there is currently insufficient evidence to support these therapies in consensus guidelines.
The rationale for therapy is context-dependent. For acute disease, the goal of treatment is to control infection and associated inflammation. This has typically been accomplished with bowel rest and antibiotics for uncomplicated disease. In certain non-severe, uncomplicated cases, diverticulitis can be self-limiting and requires no medical therapy.8 For perforated disease, source control of infection and sepsis management, when relevant, are the primary goals. Source control may include percutaneous drainage for abscess, and for purulent or feculent spillage, colectomy with abdominal washout may be necessary.
For chronic disease, management is on an elective basis. The rationale for surgical intervention is predicated on achieving one of three goals, depending on the clinical scenario: (1) prevention of future recurrences in a high-risk patient or someone with multiple prior episodes; (2) treatment of long-term complications such as fistula or stricture; or (3) definitive therapy for refractory disease that has been unresponsive to medical management. Ultimately, the goal of surgical excision is to cure the patient of diverticular disease.
There are three types of patients that are likely to most benefit from surgical excision for diverticular disease: First, patients that are immunocompromised or have significant medical comorbidities. These patients are at higher risk of serious complications from diverticular infection in the event of a recurrence; second, patients who have experienced multiple recurrences of diverticulitis and are therefore at increased risk of future episodes; third, patients who previously experienced complicated diverticulitis with an abscess that required percutaneous drainage. These patients are at increased risk for recurrent complicated disease, potentially resulting in significant morbidity or mortality. Finally, contraindications to surgery are generally limited to individuals with significant medical comorbidities, e.g. cardiopulmonary disease, that precludes them from undergoing general anesthesia.
As we have shown in this video, the main procedural steps for this operation are as follows: (1) mobilize the descending colon in a lateral to medial fashion; (2) mobilize the transverse colon and splenic flexure by taking down the gastrocolic attachments; (3) take down the peritoneal reflection and mobilize the rectum; (4) ligate the inferior mesenteric artery (IMA) and left colic artery; (5) transect the rectum with an EndoGIA stapler and extracorporealize the colon to perform the proximal transection; and (6) perform an EEA colorectal anastomosis with endoscopic leak test. This approach to the LAR results in extensive mobilization of the proximal colon, allowing for a large resection with subsequent tension-free anastomosis deep in the pelvis. The blood supply for the colonic conduit is dependent on the marginal artery of Drummond, which cannot be damaged during the operation.
Surgical approaches to rectosigmoid dissection have undergone significant evolution. The first published reports on rectal mobilization and resection date back to the early 1800s and involved perineal and trans-sacral approaches with high morbidity.9 The low anterior approach was described by Hartmann in 1921, and subsequent modifications for improved technique were published throughout the early 1900s. In the modern era, two main technological advancements have fundamentally changed and improved our approach to surgery of the colon and rectum. First, the development of trans-anal, circular stapling devices has allowed for efficient and effective stapled anastomoses low in the pelvis. Second, the advent of laparoscopy in the 1980s allowed for minimally invasive colorectal surgery with excellent visualization of the pelvis during the mesorectal dissection. As a result, the majority of elective sigmoid and rectal operations can be performed laparoscopically through several small anterior port sites with low morbidity and mortality and faster recovery.
The recommendation to perform elective rectosigmoid colectomy on a patient with recurrent uncomplicated diverticulitis should be individualized. After a single episode of uncomplicated disease, the risk of recurrence ranges from 12-23% with less than 6% risk of recurrent complicated disease.10 In these cases, the potential risk for complications from surgery must be balanced with the projected risk of future disease, with consideration of immune function and comorbidities. For patients with complicated disease on the first episode or multiple prior recurrences, the current recommendations are to offer an elective colon resection after resolution of the most recent episode, given the increased risk of recurrence.11 After surgical resection for sigmoid diverticulitis, there is an approximately 15% chance of recurrence with a 10-20% risk of postoperative complications.3
There are several active areas of investigation that may improve our understanding and treatment of diverticulitis going forward. These areas include the gut microbiome, genetic factors, diet and lifestyle, and chronic inflammatory signaling. More effective medical therapies might help to improve surgical outcomes by reducing disease severity, thereby mitigating adverse operative conditions at the time of surgery.
- Operative time: 90 minutes
- Estimated blood loss: 50 mL
- Fluids: 1200 mL crystalloid
- Length of Stay: Discharged from hospital to home without services on postoperative day 2
- Morbidity: no complications
- Final pathology: sigmoid diverticulitis
- Veress needle
- Laparoscopic ports: 12 mm x2, 5 mm x2
- Laparoscope: 10-mm 30 degree
- Covidien laparoscopic harmonic scalpel
- Endo GIA™ 30 mm Reload with Tri-Staple™ Technology
- Covidien end-to-end anastomotic (EEA) stapler
Nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
We would like to thank Theresa Kim, MD for assisting in this operation.
Citations
- Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, Gangarosa LM, Thiny MT, Stizenberg K, Morgan DR, Ringel Y, Kim HP, DiBonaventura MD, Carroll CF, Allen JK, Cook SF, Sandler RS, Kappelman MD, Shaheen NJ. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 2012;143:1179-87 e3. https://doi.org/10.1053/j.gastro.2012.08.002
- Painter NS, Burkitt DP. Diverticular disease of the colon: a deficiency disease of Western civilization. Br Med J. 1971;2:450-4. https://doi.org/10.1136/bmj.2.5759.450
- Strate LL, Morris AM. Epidemiology, Pathophysiology, and Treatment of Diverticulitis. Gastroenterology 2019;156:1282-98 e1. https://doi.org/10.1053/j.gastro.2018.12.033
- Oberkofler CE, Rickenbacher A, Raptis DA, Lehmann K, Villiger P, Buchli C, Grieder F, Gelpke H, Decurtins M, Tempia-Caliera AA, Demartines N, Hahnloser D, Clavien PA, Breitenstein S. A multicenter randomized clinical trial of primary anastomosis or Hartmann's procedure for perforated left colonic diverticulitis with purulent or fecal peritonitis. Ann Surg. 2012;256:819-26; discussion 26-7. https://doi.org/10.1097/SLA.0b013e31827324ba
- Regenbogen SE, Hardiman KM, Hendren S, Morris AM. Surgery for diverticulitis in the 21st century: a systematic review. JAMA Surg. 2014;149:292-303. https://doi.org/10.1001/jamasurg.2013.5477
- Ritz JP, Lehmann KS, Frericks B, Stroux A, Buhr HJ, Holmer C. Outcome of patients with acute sigmoid diverticulitis: multivariate analysis of risk factors for free perforation. Surgery. 2011;149:606-13. https://doi.org/10.1016/j.surg.2010.10.005
- Bharucha AE, Parthasarathy G, Ditah I, Fletcher JG, Ewelukwa O, Pendlimari R, Yawn BP, Melton LJ, Schleck C, Zinsmeister AR. Temporal Trends in the Incidence and Natural History of Diverticulitis: A Population-Based Study. Am J Gastroenterol. 2015;110:1589-96. https://doi.org/10.1038/ajg.2015.302
- Stollman N, Smalley W, Hirano I, Committee AGAICG. American Gastroenterological Association Institute Guideline on the Management of Acute Diverticulitis. Gastroenterology. 2015;149:1944-9 https://doi.org/10.1053/j.gastro.2015.10.003
- Inoue Y, Kusunoki M. Resection of rectal cancer: a historical review. Surg Today. 2010;40:501-6. https://doi.org/10.1007/s00595-009-4153-z
- Hall JF, Roberts PL, Ricciardi R, Read T, Scheirey C, Wald C, Marcello PW, Schoetz DJ. Long-term follow-up after an initial episode of diverticulitis: what are the predictors of recurrence? Dis Colon Rectum. 2011;54:283-8. https://doi.org/10.1007/DCR.0b013e3182028576
- Feingold D, Steele SR, Lee S, Kaiser A, Boushey R, Buie WD, Rafferty JF. Practice parameters for the treatment of sigmoid diverticulitis. Dis Colon Rectum. 2014;57:284-94. https://doi.org/10.1097/DCR.0000000000000075
Procedure Outline
Table of Contents
- Infraumbilical Incision, Veress Needle Insertion, and Inflation
- Trocar Placement
- Port Placement
- Freeing Omentum from Abdominal Wall
- Descending Colon and Splenic Flexure Mobilization
- Sigmoid Colon Mobilization
- Isolation and Division of IMA Pedicle
- Division of Lateral and Posterior Stalks
- First Bowel Division
- Isolation and Division of Marginal Artery
- Second Bowel Division
- Anvil Placement and Abdominal Closure
- Baker-Type Anastomosis
- Water-Immersion Sigmoidoscopy
- Subcuticular Suture
Transcription
INTRODUCTION
Hi, I’m Dave Berger. I’m one of the surgeons here at Mass General, and today’s first case is going to be a case for a woman who has recurrent diverticulitis. She’s had about 12 episodes in the last year and a half, 2 years. And so, we’re going to do an elective resection of that segment for her. The basics of the procedure – it’s going to be laparoscopic and we’re going to begin by placing our ports. Once we have established that, we’re going to go in and get into the lesser sac. We’re going to use that to take down the splenic flexure. We’re then going to proceed to take the descending colon and sigmoid colon off from where it’s stuck to the sidewall. Once we’ve completely mobilized the colon, we’ll divide the left colic vessels with the Harmonic Scalpel and then we’ll isolate the IMA pedicle. We’ll take the IMA pedicle either with a stapler or with clips, depending on the size of the vessel. Once we’ve accomplished that, we’ll enter the pre-sacral space and mobilize the rectum up. We’ll then divide the posterolateral stalks with the harmonic scalpel and we’ll divide the rectum itself using a stapler. Once I have achieved that, I’ll make a small hole usually peri-umbilically and bring the bowel out. I’ll divide the marginal artery, and then I’ll divide the bowel proximally. And once I’ve done that, I’ll place an anvil through the lateral aspect on the anti-mesenteric border of the bowel. Then I’ll drop that back into the abdominal cavity. I’ll close and then we’ll re-insufflate and laparoscopically complete a side-to-end Baker type anastomosis between the descending colon and the rectum. Once we’ve completed that, we will close our incisions and the operation will be done.
CHAPTER 1
Yeah, I know. You set the level. Put on Pandora. Put on Traffic.
We’re going to do a laparoscopic low anterior resection for diverticular disease. Alright gas on please.
CHAPTER 2
Ok we've now entered the abdomen. Now we're going to place our ports for the surgery. So our first port goes in the left lower quadrant and that’s a 5mm port. So the first thing we're going to do is we're going to lift the omentum up and we're going to get into the lesser sac. Now in some of these cases of diverticular disease, the omentum is stuck in the left lower quadrant and that is the case here. So before we can even begin, I've got to free this piece of omentum up. And these are adhesions because of the diverticulitis or current bout of diverticulitis, but if I don't free this up, I can't flip the omentum up, and thus I can't enter the lesser sac, so that has to be our first task. We’re done with that. You got that, I got this. So now that that's free. What a bummer. Unfortunately, we got the blood now right. So now I'm rolling the omentum up and we're going to find the upper aspect of the colon appear.
I want to keep moving out in that plane right there. Can you vent the…Go clean your camera, wipe it on the liver. We’re working into the lesser sac, right here, right? Ok come right up in here. Bring your camera in a bit. Yup. Of course she has a very, very stuck colon. We’ll get that there.
That's way too much light. Right here. Get a bite right there. Right there. So we're going up now the side up along the descending colon. Free that up from where it's attached to the sidewall out there. So, those are adhesions right from the diverticular disease. In order to take down the flexure we need to get these all down. You can see the spleen coming into view back there right, so now if we come back here, we’re now going to keep walking up this plane here.
[Resident]: Lateral ligament right?
Well there's no lateral ligament. Well, it’s the area where the colon is stuck to the side right there. Keep walking up - too lateral - yup.
So now we’re going to be able to see; there's an attachment to the spleen, take that down. That's a little unusual to see a direct attachment like that. Take those bands right there.
Ok so we got to go right here. Right there.
These ones are really hard, right. They’re much, much harder. Ok, so you can see where you're stuck there right? See the plane now? Closer to the bowel. Yup. Higher up - yup. Yup right there. Don't do that. Get it out with the camera. So we're good there and we need to now come through here. You’re not showing me anything. Alright so you’re going to go right under here. We’re going to go right here, right? What we're going to do is we're going to stay off of the retroperitoneum, right?
You have to be really careful on these because she's super skinny. We're going to come right here. Don’t twist. Right here, closer to the bowel. She's so thin that you're having so much difficulty keeping the camera clean and everything.
[Resident]: Oh is that what it is?
Well there's just no space right? It's a domain issue. See how I'm just rolling that out of the retroperitoneum.
Alright so now we're pretty darn free. So you can see that we're stuck here. Now, the good thing to see about this so far is that we're definitely out of plane, in that we're deep and this is the diverticular area right here, right?
[Resident]: Just in that one spot though.
Yeah I know we're just, yeah. The ureter’s right there, see it? Right there. See it moving? Not as clean as we want to be. Alright. Take this, look right here. Look, lift your hand off this. So because she’s so thin, you have to be doubly careful down in here, right? Because the plane is super, super thin. You can see.
[Resident]: Oh that’s the tubule…
Right and so, we can see how we've raised up more stuff than we want to, right?
[Resident]: And is that, ureter down there?
Well you got to show me up here. Because these planes are just paper, right?
[Resident]: Yeah.
So you can take that there. And you can see how ridiculously redundant the bowel is, right?
[Resident]: Yeah.
That makes it much harder to do. So now we've got to take some left colic vessels to free this up. So we're going to go in here and take the left colic vessels. You're getting a lot of haze in the picture because the balloon is small. So laparoscopy is like operating on a ship in a bottle and so when the bottle is very small, what happens is it just gets much, much harder, in terms of, you know everything, so it's the very skinny person that makes it hard.
[Resident]: Is it unusual for someone?
Well in most areas of surgery, skinny is good right? Lower. In laparoscopy skinny is not.
Ok so that's the last of the flexure, now that's all down. Now let's just see up here, what we need to do to make this free completely. So we can bring it down. So that band, see that little band right there? Ok, see the band right there yeah. See, all that does is allow that to come down right? You're freeing it off the edge of the pancreas. So now we're going to move positions so we can operate down into the pelvis. Ok take that band there, that's an adhesion to the small bowel.
So you see the ureter right there. Let’s see if we can grab it, show them that it moves. See the ureter? That’s the ureter.
Surgeons will like that, otherwise it doesn't make much difference. You can see that it runs back here, show me back here. So that same ureter runs here. Right there. Now, you got to flip this over again. Show me up here now. Show me where we’re stuck.
So this is the IMA pedicle right here. Let’s see, I think we can open a 12 sleeve instead of a 15, guys. Can I have that for a sec? A sleeve is the this - the sheath that we use to do the laparoscopy. And what I’m doing now is, I think I’m going to be able to take the IMA with clips, so I’m just skinnying off the pedicle. Knife.
So now, I’m just going to upsize my 5 port to a 10-12. And now I’m going to use clips to take the vessel. You can see the vessel right there. Another clip. That’s the IMA, yeah. In a heavy person it’s pretty hard for me to do it with clips because the lymphatics and surrounding tissue is too thick. But in a relatively thin person, I can usually do it with clips. Clip.
So what I'm doing is I'm clipping the lower end and the upper end and I'm using a harmonic simply to divide it.
You can see the artery pulsating right there.
CHAPTER 3
So now our bowel is free. So now, the next thing we’re going to do is we’re going to figure out where we need to take the bowel. The bad diverticular disease is here in the sigmoid colon. You can see how thick that is. So now, we’re going to go down towards the rectum, and we’ve elevated the rectum up, and we’re going to look for where the taenia coalesce. Show me the rectum please, pull back, lift your hand up. And you can see that the taenia are coming together here, so we’re going to go actually right here. So the next thing I’m going to do is divide the lateral and posterior stalks, and I do that with the harmonic scalpel as well. Let’s see if I can bend it here too. And now once again, I’m diving out the lateral, posterior and lateral stalks so that I get to normal bowel.
I'm going to use a 63.5 guys. Alright so now I got that nice and free. Stapler?
So now what I’m going to do is divide the bowel. Pull your camera back. She is really petite huh? That really makes it a lot harder to do laparoscopically unfortunately. So now I’m going to divide the bowel with the stapler and I’m just positioning the bowel in the center of the stapler.
Bummer, that’s not going to divide it all, I don’t think. Yeah ok so that’s just fat, see it? Ok so now we’ve divided the bowel out. Tooth grasper. And now what I’m going to do is grab it and bring it out through the abdominal wall. No I don’t have it. Ok. Lights on please. Can I have the knife for a second please. Ok so now what we’re going to do is extend my incision around the belly button. Ok now take your cautery. Pickups with teeth. Mhmm, schnidt. Ok so open that up. Ok can I have a Richardson please? We may need to make this a little longer, longer this way. Take that stuff there in the middle, no no, this way. Subcutaneous tissue you take around the horn and it’s the fascia we take differently, right? Mhmm straight up.
Ok you ready? So we’re going to bring the bowel up to the abdominal wall. Grab it right there with a Babcock. Ok pull it out. Ok good, let it go. That’s always a winner right there. Alright, that needs a harmonic right there. And then one more bite there. Ok so now we’re left with our colon on our marginal artery, and so what we’re going to do is choose our place to do our anastomosis. I really like to take.
[Resident]: Dr. Berger, can you see the diverticular disease from the outside?
Yeah so the thickened area where she had the problem is this right in here. See that? See how thick that is? Ok so let’s go here, cautery. That was a little bit close. Pick-ups. So now we’re going to isolate the marginal artery.
Can you take that down there? And this is the marginal artery right here. Schnidt. 3-0. ILA 100 next. Now the next thing that we're going to do is divide the bowel after we clean off the posterior side. Use your cautery. Stapler. And that leaves our specimen. And now the next thing that we're going to do is we're going to place our Anvil to do our anastomosis. Cautery. Just a little. Buzz me.
No no, we need the 3-0 double ended prolene. Stitch. So we’re going to put in a purse string of 3-0 double loaded prolene and I put it in, in a baseball fashion. Snap. Too much bowel. You want to make sure you get the mucosa and the serosa here. Backhand.
That’s a forehand shot. Ok anvil. So now that we’ve baseball-ed in our suture, we’re going to place the anvil in. And here goes the anvil going in. Good. Now we’re going to tie the anvil in place. Cut.
You’re pulling it so that it moves out of my pickups, you’re pulling too hard, right? Ok we set that in on the anti-mesenteric border. Now once that’s tied in we’re going to drop this back into the abdominal cavity and we’re going to close our hole and we’re going to go back laparoscopically. So #1 prolene please.
It’s a CT 6 needle. It’s going to be hard. So now we’re going to sew the fascia back together. Rectosigmoid is our specimen yeah.
Alright Lynn, we’re going to go gas on, lights on. We need the tube of lube.
[Nurse]: It’s not sterile.
That’s fine.
CHAPTER 4
That’s the iliac, the ureter here. Can I have a toothed grasper? Ok go ahead, wiggle in. Handle higher, keep wiggling, keep wiggling. Here you come, here you come. There you go. Now, bring your spike out. Now push your handle away from me. There you go, that’s good, stop there. Ok now bring yourself into the middle. Hold on. Bring yourself a little more into the middle. There you go. Alright now let me just make sure this is rotated properly, which it is. Now push your handle down a bit. Now bring it in. Yeah we just want to make sure we don’t pinch anything. Go ahead. No twist in that. Ok good, good. Take it, squeeze tight. I want to hear the click. Good, squeeze it again. Ok now wiggle it out, lots of wiggling, oscillating wiggling. Pull it through, good. Give me a little less Trendelenburg. That may help you.
Now the next thing we’re going to do is check our anastomosis under water. A little less Trendelenburg maybe. Good, thank you. Alright can I have a bowel grasper? Just going to occlude the upper bowel. Go ahead. Center yourself up, there you go, put air in. There you go, there’s the anastomosis. See it? Show everybody the anastomosis, there you go. And we have no bubbles so our anastomosis is air tight. Ok suck it out. Can I have some bowel graspers please?
So the next thing I’m going to do or the last thing I’m going to do is just make sure the bowel isn’t stuck in the trap under the colon. And that’s what that is, and we just flip that bowel out and now you can see that the colonic mesentery is lying straight all the way down to our anastomosis.
CHAPTER 5
Ok take your monocryl and sew that all closed. Can I have a monocryl? Ok now I want you to hold that there. Hey Chelsea you can let go.
[Nurse]: Do you still have a needle up?
I do.
So I thought that was actually, I thought that was pretty hard. The balloon was small. I think you can see a lot better in an average case. That was a good example of a hard one because she was too small. Alright thanks guys. Supine, both arms out.
I found the case to be fairly difficult due to the small size of the patient. We have very limited room to move around in the abdomen and as the patient's belly was quite small. Otherwise the case went very smoothly and we didn't have any problems and hopefully she'll do well.