
Cataract Extraction with Phacoemulsification and Posterior Chamber Intraocular Lens
Main Text
Table of Contents
Cataract is a leading cause of treatable blindness in the world. While there is a significant difference in access to surgical care in developing vs. industrial nations, cataract is a significant contributor to visual impairment in both. The diagnosis of cataract is made through assessment of visual acuity, visual disability, and slit lamp biomicroscopy. Common indications for surgery include difficulty with glare, night driving, decrease in best corrected vision impairing distance and/or near vision, and impairment of view to the retina that is precluding necessary treatment. In the US, the standard for cataract extraction has become phacoemulsification. The article demonstrates and reviews the technique of cataract extraction using phacoemulsification with intraocular lens implantation using the divide-and-conquer technique.
Patients with visually significant cataract will report some kind of visual decline or functional decline due to a loss of visual acuity. This can be as simple as a decline in best corrected visual acuity at distance and/or near, or it can be a more subtle loss of function, such as requiring more light for reading, difficulty with night driving, increasing glare with oncoming headlights, or solar glare when driving when the sun is low on the horizon. The critical information here lies with documenting a decrease or loss of daily functioning. This is the indication for surgical intervention.
Visual acuity
- Check patient's visual acuity with current correction.
- Pinhole can give a quick reference on whether or not refraction may be beneficial.
- Manifest refraction to achieve best corrected visual acuity.
Glare testing
- Brightness acuity test (BAT) is used to demonstrate glare.
- This test is useful for documenting visual impairment with glare in patients that have good best corrected visual acuity.
Potential acuity meter (PAM)
- This is a useful test in patients with comorbid ocular disease to help counsel the patients regarding the potential vision outcome postoperatively.
Slit lamp findings
- Lids and adnexa should be examined for any signs of blepharitis, which should be treated preoperatively. This will also give clues to any anatomic issues that may affect surgical exposure.
- Conjunctiva should be evaluated. This may affect the position of the corneal incision as there may be postsurgical changes from glaucoma surgery, or pterygium that may limit access to the corneal limbus.
- Cornea exam should focus on evidence of previous corneal surgery (refractive surgery or transplant procedures). Look for any scars or opacities from surgery, trauma, or infection that may impair the surgical view. Also, look for any signs of dystrophies that can affect the refractive outcome as well as predispose to endothelial decompensation postoperatively.
- Anterior chamber depth can give you a sense of how much space you will have to work. Short eyes with shallow chambers will have phacoemulsification done slightly more posteriorly in order to limit endothelial damage.
- Iris should be assessed for pupil dilation, transillumination defects, and pseudoexfoliation material. These are important for the assessment of surgical exposure as well as potential loss of stability of the capsular lens complex. Noting any signs of trauma, zonular compromise, and/or poor dilation will help in surgical planning. Surgeon may decide to have specialty devices available to facilitate surgery including iris hooks, Malyugin rings, capsular hooks, and capsular tension rings and segments.
- Lens should be assessed for lens opacity. The capsule and zonular support should also be assessed. Look for centration of the crystalline lens. Assess the stability of the lens. Focus should be on any sign of capsular violation or compromise. This could be congenital, traumatic, or iatrogenic. This is true also for zonular loss. Presence of any of these factors can affect the surgical approach. In patients with significant disruption, pars plana lensectomy may be the safest approach.
- Dilated exam should be performed. This will help facilitate the evaluation of the lens. Also important is the evaluation of the retina and optic nerve. This will help determine if there are other diseases that are affecting the vision, and whether cataract surgery would be beneficial or if other treatment may be needed.
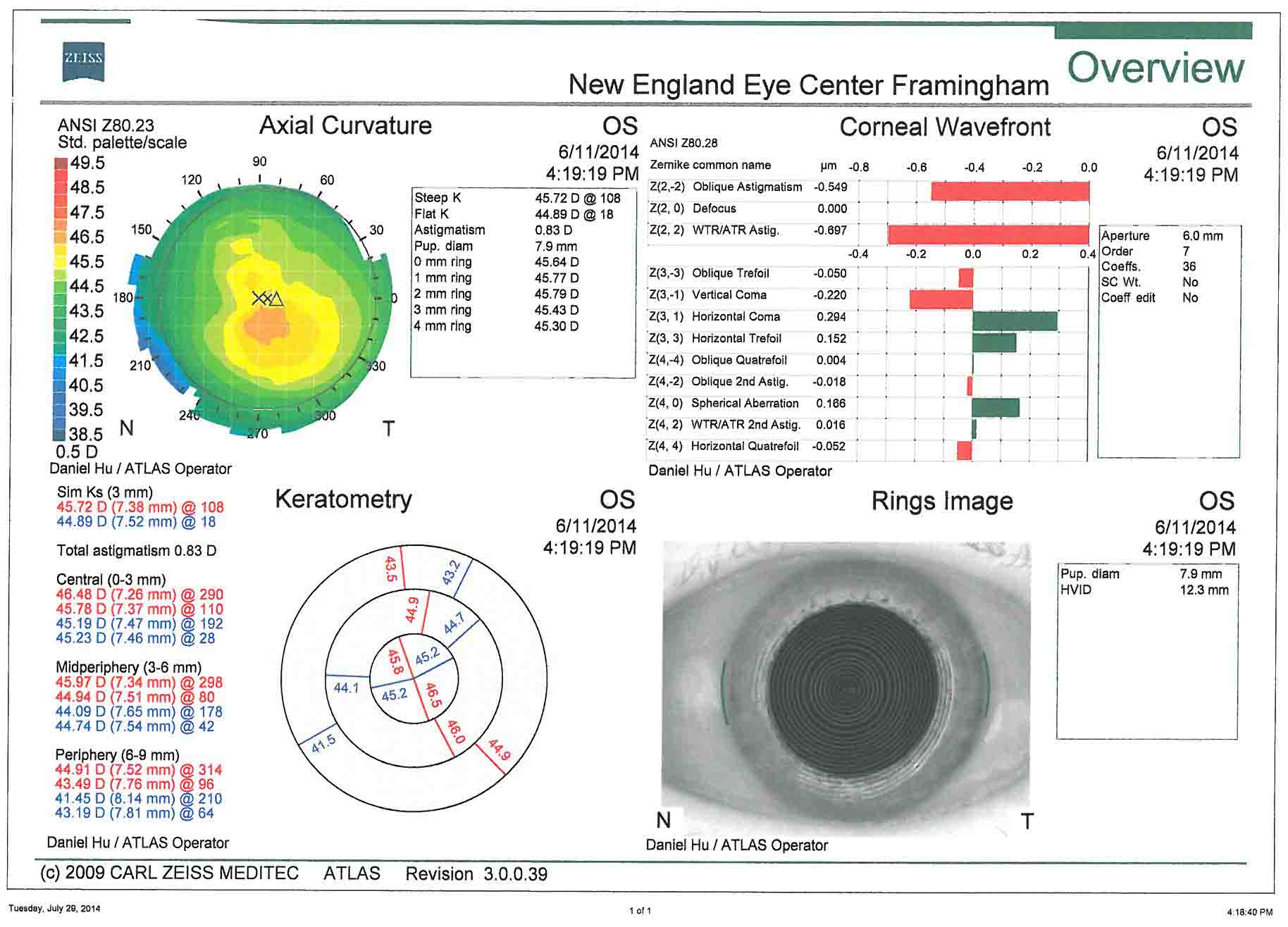
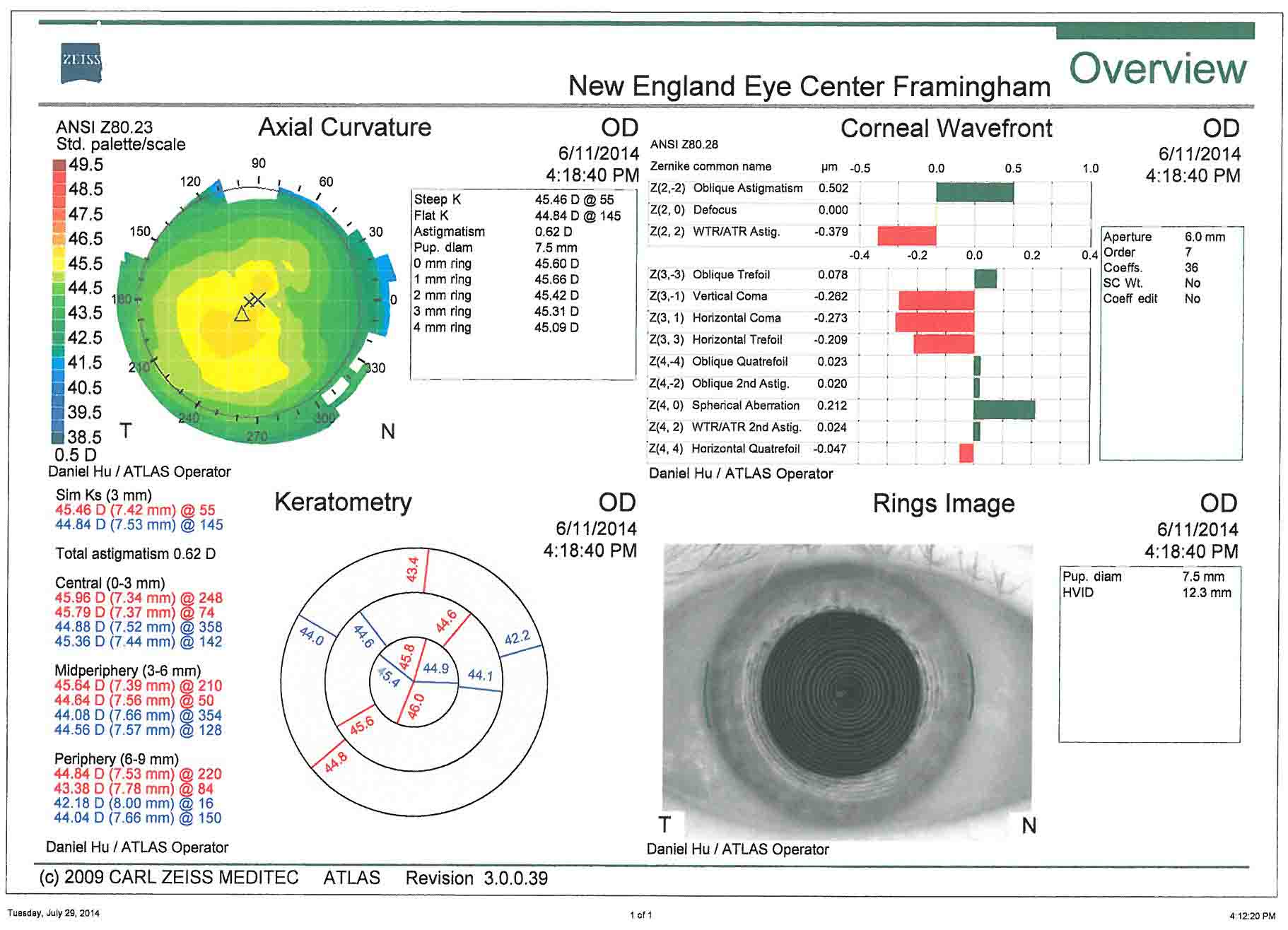
- Corneal topography- This is useful for the assessment of preoperative corneal astigmatism. Surgical planning of astigmatism management is based off of these images.
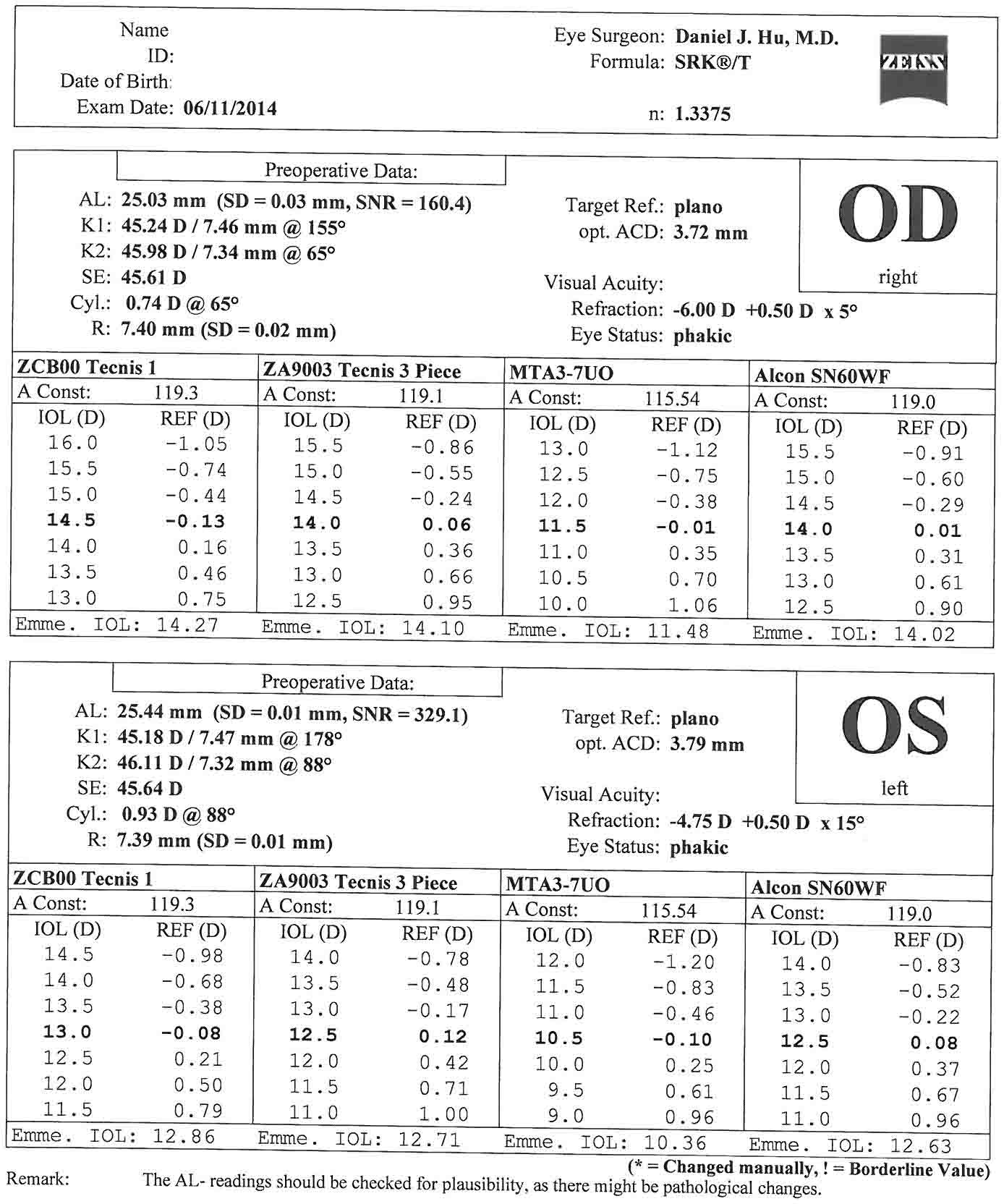
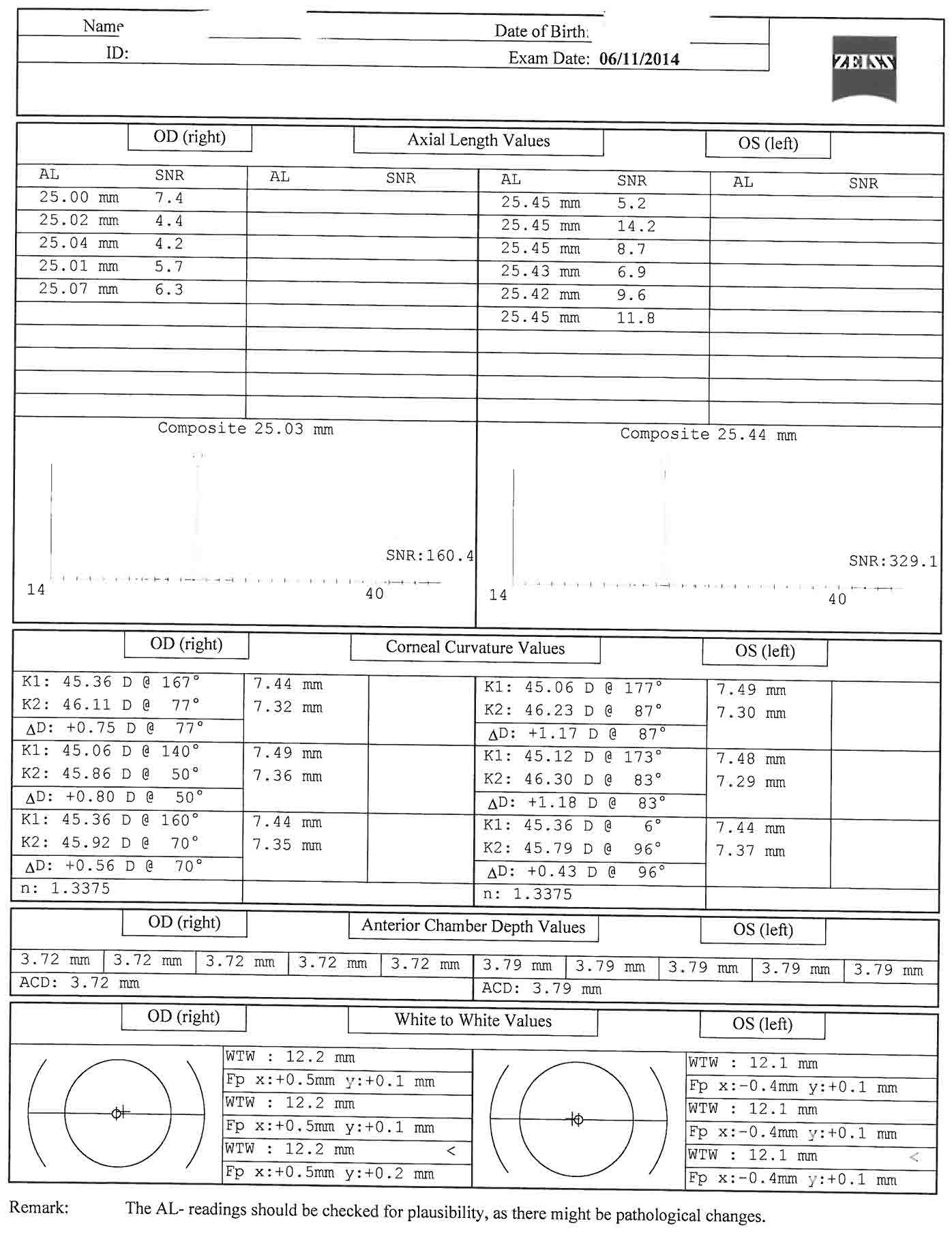
- Biometry (IOL master)- Keratometry, anterior chamber depth, white-to-white, and axial length are measured, and intraocular lens powers calculated.
- B-scan- In cases of mature cataract that impairs the view to the retina. This allows a gross assessment of retinal anatomy. Is there a retinal detachment or mass present?
- Specular microscopy- Can be performed in cases of endothelial dysfunction to assess endothelium prior to surgery.
In this case, there is less than 1 diopter of oblique corneal astigmatism in both eyes. This corroborates well with the keratometry from the biometry. In this case, corneal relaxing incisions could be used to manage the astigmatism. The patient has elected to forgo astigmatism treatment.
- If left untreated, cataract will lead to progressive vision loss and blindness.
- If the cataract is visually significant, there are limited options for treatment. Surgical intervention is necessary in order to restore vision.
- Phacoemulsification using divide-and-conquer has the advantage of being a universal technique that can be used for all degrees and types of cataract.
- Special consideration should be taken in cases of dense, mature nuclear sclerosis, zonulopathy, subluxation of the crystalline lens, or any cases with a limited view of the anterior segment.
Potential postoperative complications include the following conditions:
- Corneal edema
- Descemet's membrane detachment
- Induced astigmatism
- Corneal wound burn
- Wound leak
- Epithelial downgrowth
- Toxic anterior segment syndrome (TASS)
- Intraoperative floppy iris syndrome (IFIS)
- Iridodialysis
- Cyclodialysis
- Urrets-Zavalia syndrome
- Elevated intraocular pressure
- Malignant glaucoma
- Retained lens material
- Capsular rupture
- Vitreous prolapse
- IOL complications (decentration and dislocation, pupillary capture, capsular block syndrome, uveitis-glaucoma-hyphema syndrome, pseudophakic bullous keratopathy, incorrect IOL power, IOL glare, IOL opacification)
- Anterior capsular fibrosis and phimosis
- Posterior capsular opacification
- Hemorrhage (retrobulbar hemorrhage-complication for retrobulbar anesthesia, suprachoroidal effusion, expulsive suprachoroidal hemorrhage, hyphema)
- Chronic postoperative uveitis
- Endophthalmitis
- Cystoid macular edema
- Retinal light toxicity
- Macular infarction
- Retinal detachment
Cataract surgery has undergone considerable advancement over the last several decades that has improved the safety and efficacy of the procedure. This has been driven by a progressive movement toward decreasing surgical trauma to the eye. Modern cataract surgery has progressed from large incision techniques, such as intracapsular cataract extraction, to extracapsular cataract extraction, to now small incision phacoemulsification.1 Cataract surgery has become an exceptionally safe and successful surgical procedure. Multiple large studies have shown best corrected postoperative visual acuity of 20/40 or better in 85.5–89% of all patients, and 94.7–96% of patients without preoperative ocular comorbidities. 95% of patients were satisfied with the outcome of their surgery.2-4 However, there continue to be challenges regarding the reproducibility of the capsulotomy, the use of ultrasound and its effects on the corneal endothelium, as well as capsular complications. As the risk of significant intraoperative complications has been reduced, the expectation for visual outcomes has continued to increase. Cataract surgery and refractive surgery are increasingly linked as outcomes are being driven by the expectation of emmetropia.
Cataract surgery continues to evolve away from manual surgery to technology driven techniques. A major leap forward was the advent of phacoemulsification by Charles Kelman, MD in the 1960s. By the 1990s, phacoemulsification had become the standard for cataract surgery in developed countries. Refinements in phacoemulsification have continued to improve outcomes and decrease complications. Femtosecond laser-assisted cataract surgery is the newest technology to be incorporated into use with cataract surgery. The potential benefits of femtosecond laser-assisted cataract surgery include reproducible capsulotomy, reduction in ultrasound time, and reproducible corneal incisions. A significant reduction in ultrasound time has been shown. Femtosecond lasers have also been shown to have improved accuracy and reproducibility of capsulotomy and corneal incisions. The reproducibility of the corneal incisions is especially valuable in the context of astigmatism control.5-8 The intended benefits of these characteristics is to improve patient recovery time, reduce complications, and help achieve better refractive outcomes.
As cataract techniques have improved, so has the expectation for rapid postoperative recovery, as well as immediate refractive outcomes. Improved biometry has increased the predictability of postcataract surgery outcomes. Intraoperative aberrometry has been a tremendous asset in helping with the accuracy of IOL selection, especially in eyes with previous keratorefractive surgery.9 This predictability is critical when considering the refractive expectations of both postrefractive surgery cataract patients, and combined refractive-cataract surgery patients who are expecting immediate outcomes.
The emmetropic eye with adaptation for presbyopia has become the goal of many patients. While there is still room for this technology to mature, current technology is able to achieve this for many patients. Astigmatism can be managed at the time of surgery with on axis surgery, corneal relaxing incisions, or toric intraocular lenses.10-13 Presbyopia can be managed with monovision, multifocal, or accommodating IOLs.14-15 These advanced intraocular lenses have given patients the ability to function with greater freedom from the use of spectacle correction for the majority of their daily tasks. Advances in IOL technology will continue to drive the desire for spectacle independence postoperatively.
- Corneal topographer- Zeiss Atlas 9000
- Biometry- Zeiss IOL Master
- Phacoemulsifier- Alcon Infiniti Vision System
- Settings
- Sculpt: Irrigation: 95 cm, Torsional: 100 (Linear), Vacuum: 90 mmHg (Linear), Aspiration: 22 cc/min (Fixed)
- Quadrant: Irrigation: 100 cm, Torsional: 100 (Linear), Vacuum: 350 mmHg (Fixed), Aspiration: 40 cc/min (Linear)
- Epinucleus: Irrigation: 95 cm, Torsional: 95 (Linear), Vacuum: 300 mmHg (Linear), Aspiration 30 cc/min (Linear)
- Cortex: Irrigation: 100 cm, Vacuum 500 mmHg (Linear), Aspiration: 35 cc/min (Linear)
- Polish: Irrigation: 95 cm, Vacuum 10 mmHg (Linear), Aspiration: 6 cc/min (Linear)
- Viscoelastic: Irrigation: 95 cm, Vacuum 600 mmHg (Linear), Aspiration: 40 cc/min (Fixed)
- Surgical microscope- Leica
- Intraocular lens- AMO Tecnis ZCB00 Intraocular lens
The author has no financial relationships with any of the products or equipment mentioned in this article.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Stein JD. Serious adverse events after cataract surgery. Curr Opin Ophthalmol. 2012;23(3):219-225. doi:10.1097/ICU.0b013e3283524068.
- Lundström M, Barry P, Leite E, Stenevi U. 1998 European cataract outcome study: report from the European Cataract Outcome Study Group. J Cataract Refract Surg. 2001;27(8):1176-1184. doi:10.1016/S0886-3350(01)00772-6.
- Lum F, Schein O, Schachat AP, Abbott RL, Hoskins HD Jr, Steinberg EP. Initial two years of experience with the AAO National Eyecare Outcomes Network (NEON) cataract surgery database. Ophthalmology. 2000;107(4):691-697. doi:10.1016/S0161-6420(99)00184-0.
- Jaycock P, Johnston RL, Taylor H, et al. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye (Lond). 2009;23(1):38-49. doi:10.1038/sj.eye.6703015.
- Reddy KP, Kandulla J, Auffarth GU. Effectiveness and safety of femtosecond laser-assisted lens fragmentation and anterior capsulotomy versus the manual technique in cataract surgery. J Cataract Refract Surg. 2013;39(9):1297-1306. doi:10.1016/j.jcrs.2013.05.035.
- Abell RG, Kerr NM, Vote BJ. Toward zero effective phacoemulsification time using femtosecond laser pretreatment. Ophthalmology. 2013;120(5):942-948. doi:10.1016/j.ophtha.2012.11.045.
- Hatch KM, Talamo JT. Laser-assisted cataract surgery: benefits and barriers. Curr Opin Ophthalmol. 2014;25(1):54-61. doi:10.1097/ICU.0000000000000013.
- Roberts TV, Lawless M, Chan CCK, et al. Femtosecond laser cataract surgery: technology and clinical practice. Clin Exp Ophthalmol. 2013;41(2):180-186. doi:10.1111/j.1442-9071.2012.02851.x.
- Ianchulev T, Hoffer KJ, Yoo SH, et al. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology. 2014;121(1):56-60. doi:10.1016/j.ophtha.2013.08.041.
- Wang L, Misra M, Koch DD. Peripheral corneal relaxing incisions combined with cataract surgery. J Cataract Refract Surg. 2003;29(4):712-722. doi:10.1016/S0886-3350(02)01838-2.
- Kaufmann C, Peter J, Ooi K, et al. Limbal relaxing incisions versus on-axis incisions to reduce corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg. 2005;31(12):2261-2265. doi:10.1016/j.jcrs.2005.08.046.
- Sheppard AL, Wolffsohn JS, Bhatt U, et al. Clinical outcomes after implantation of a new hydrophobic acrylic toric IOL during routine cataract surgery. J Cataract Refract Surg. 2013;39(1):41-47. doi:10.1016/j.jcrs.2012.08.055.
- Visser N, Bauer NJC, Nuijts RMMA. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39(4):624-637. doi:10.1016/j.jcrs.2013.02.020.
- Schmickler S, Bautista CP, Goes F, Shah S, Wolffsohn JS. Clinical evaluation of a multifocal aspheric diffractive intraocular lens. Br J Ophthalmol. 2013;97(12):1560-1564. doi:10.1136/bjophthalmol-2013-304010.
- Cumming JS, Colvard DM, Dell SJ, et al. Clinical evaluation of the Crystalens AT-45 accommodating intraocular lens: results of the U.S. Food and Drug Administration clinical trial. J Cataract Refract Surg. 2006;32(5):812-825. doi:10.1016/j.jcrs.2006.02.007.
- Gimbel HV. Divide and conquer nucleofractis phacoemulsification: development and variations. J Cataract Refract Surg. 1991;17(3):281-291. doi:10.1016/S0886-3350(13)80824-3.
Cite this article
Daniel J. Hu, MD. Cataract extraction with phacoemulsification and posterior chamber intraocular lens. J Med Insight. 2023;2023(7). https://doi.org/10.24296/jomi/7Procedure Outline
Table of Contents
- Pre-op holding
- Intravenous sedation - Remifentanil
- Peribulbar block with 50/50 mix of 2% lidocaine and 0.75%
- Honan balloon is placed for 5-10 minutes
- Intraoperative
- Intravenous midazolam
- Patient is transferred to surgical eye bed and placed in supine position
- Surgical site is prepped with 5% povidone-iodine. A drop is placed on the ocular surface and the periocular skin and lids are prepped
- Aperture drape placed over operative eye
- Small Tegaderm cut in half to drape eye lashes of the upper and lower lid
- Lid retraction with angled wire Lieberman speculum
- Balanced salt solution for irrigation throughout the case to maintain surgical view
- Paracentesis
- 1.1-mm side port blade (1.1-mm Clearport-Sharpoint) is used to create paracentesis tract parallel to iris plane approximately 3-4 clock hours from the main incision
- Intracameral injection of dispersive viscoelastic (Viscoat-Alcon) to pressurize eye
- Temporal clear corneal incision
- 2.5-mm keratome (2.5-mm angled slit, bevel up keratome blade-Sharpoint) is used to create a triplanar corneal incision just anterior to the surgical limbus
- Capsulotomy
- 27 gauge cystotome on cohesive viscoelastic is used to create the initial capsulotomy and capsular flap
- The purpose of the cohesive viscoelastic is to control the tear if needed. If the capsular tear is going radially toward the equator of the lens, some viscoelastic injected over the tear can immediately gain control of the radial tear and allow the surgeon to recover the capsulotomy
- The anterior capsule is punctured centrally
- The capsular tear is propagated toward the 9 o'clock direction with a slight “smile” configuration that helps to facilitate a controlled flap toward the 12 o'clock direction
- Continuous curvilinear capsulorhexis
- Utrata forceps are then used to grasp the capsular flap, and in a clockwise fashion, complete a continuous curvilinear capsulorhexis
- The clockwise direction of the tear allows for completion of approximately 75% of the capsulorhexis before reaching the sub-incisional capsule. This technique allows for a significant amount of capsule to be available to help facilitate the capsulorhexis through the sub-incisional space
- Hydrodissection and hydrodelineation
- Balanced salt solution on a flat cannula is injected under the anterior capsule to separate the cortex from the epinucleus and nucleus of the cataract
- This step is critical in allowing free rotation of the lens nucleus for nuclear disassembly
- A fluid wave should be visible as the BSS separates the nucleus from the cortex and capsule
- Hydrodelineation is seen here as well. This creates another separation between the epinucleus and nucleus. The golden ring sign can be seen. The epinuclear shell can be another barrier of protection for the posterior capsule during nuclear disassembly.
- The BSS cannula is used to rotate the lens nucleus to confirm mobility
- Phacoemulsification
- Phacoemulsification handpiece (30-degree mini-flared Kelman ABS tip) is then placed through the temporal corneal incision
- Minimal central cortical cleanup is performed. This will leave longer cortical tags. This will be useful during cortex removal later in the case
- Phacoemulsification in scolpt is used to create a central groove essentially demarcating 2 heminuclei. The groove should be deepest where the cataract is largest in anterior posterior dimension. Care should be taken not to groove deeply in the periphery as the A/P dimension of the lens is less, and the posterior capsule can be more easily encountered
- Grayson Nucleus manipulator is then placed through the paracentesis deep into the groove along with the phaco tip. Using minimal pressure posteriorly to keep the instruments at the base of the groove, the Grayson and phaco tip are separated, splitting the nucleus into 2 heminuclei
- Lens nucleus is rotated with the Grayson, and the heminucleus is grooved and cracked in similar fashion. This is repeated with the second heminucleus
- Quadrant removal settings are then used to remove the 4 lens quadrants
- Phaco is performed at the iris plane, which provides a safe distance from both the capsular bag and the corneal endothelium
- Epinucleus is removed with the phaco handpiece
- Cortical removal
- Cortical remnants are removed with coaxial irrigation/aspiration handpiece (silicone sleeve straight I/A tip). Linear aspiration instead of fixed aspiration allows for controlled purchase of the cortical material, especially sub-incisional
- Sub-incisional cortex is the first to be removed. This is where leaving a cortical tag allows for easier removal of cortex. Straight I/A tip is rotated with aspiration port rotated posteriorly to purchase the cortical tags sub-incisionally. This is done with minimal wound distortion. After purchase of the cortical tag, the aspiration port is rotated anteriorly into the central safe zone to complete aspiration of that cortical material
- The remaining cortex can be removed with the aspiration port placed under the anterior capsular edge, again polling towards the central safe zone
- Capsular polish
- Nightingale capsular polisher is used to clear the posterior capsule of any residual lens epithelium
- This is inserted through the temporal incision while the capsular bag is deflated
- This allows for the Nightingale to rub off any adherent lens debris
- Inflation of capsular bag
- Cohesive viscoelastic is injected into the capsular bag to create space for injection of the IOL
- Injection of posterior chamber IOL
- Wound-assisted technique using the Platinum 1 injector
- The IOL is injected with the leading haptic aimed into the capsular bag
- Trailing haptic is placed into the capsular bag with a Kuglen hook
- The haptics are left in the 3- and 9-o'clock position
- Removal of viscoelastics
- Irrigation-aspiration handpiece is used to aspirate the viscoelastic in the capsular bag and anterior chamber
- Reform the anterior chamber with balanced salt solution
- BSS is injected in the temporal incision while hydrating the corneal stroma
- This helps to seal the corneal incision
- Paracentesis is also hydrated
- The eye is left with intraocular pressure of about 15-20 mmHg
- Gentle pressure is placed at the posterior wound edge to test for wound stability and leakage
- Suture if necessary
- If the wounds are not water tight, then interrupted 10-0 nylon suture is placed in the wound. Knot is rotated and buried
- Remove lid speculum
- Immediate postoperative care
- Dress eye with antibiotic/steroid ointment, soft eye patch and hard shield
- Topical antibiotic, non-steroidal, and steroid eye drop 4 times a day for 1 week, then non-steroidal and steroid eye drop twice a day for 3 weeks.
- Eye shield at bedtime for 1 week
- Limited physical activity for 1-2 weeks
- Follow-up appointments at 1 day, 1 week, and 1 month post-op
- Post-op refraction at 1 week
Transcription
CHAPTER 1
I am Daniel Hu.I am an assistant professor of ophthalmologyat Tufts University School of Medicine andthe New England Eye Center, Tufts Medical Center.And today we will be talking aboutcataract extraction using phacoemulsificationwith implantation of the posterior chamber intraocular lens.After prepping and draping the patient,you know, we- I like to use a Lieberman speculumto, you know, keep the lids open.And then we'll create a paracentesisto access the anterior chamber.And we'll fill the anterior chamber with viscoelastic,and then we'll use a keratome blade tocreate the main incision.Then with a cystotomeand Utrata forceps, we'll createthe capsulotomy. We'll hydrodissectand hydrodelineate the lens nucleus.We'll then fragment the lens nucleuswith a phacoemulsification handpiece.Then remove the cortical remnantswith automated irrigation aspiration.We will then inject theintraocular lens and the capsular bag,and remove any remaining viscoelastic materials.And then check the wounds,seal everything up, and-the case is done.I'll be showingthe divide and conquer technique.I believe it's-one of the easier techniquesto learn for beginning surgeons.One of the benefits of it isthat it can be very gentleto the capsular bag if done properly.And doing socreates very little zonular stressand, I think, lowersthe potential risk for complications.So it's a very safe and gentle procedure.We'll be doing surgery today with\Nan Alcon Infiniti machine,and we'll be using a 2.5-mm incision,and for my second instrument,\NI'll be using a Grayson spatula.I like to use that instrument because it'sgot sort of a wide, flat end to it without any sharp edges.So, for this particular technique, it's particularly usefulbecause I wont be needing to be doing any choppings.Primarily, I'll be using it for lens manipulation, rotation, and splitting,and so it's an excellent instrument for that purpose.
CHAPTER 2
So here, in my right hand I have a0.12 clear B forcepsto stabilize the globe.I have a 1.1-mm side port bladeto create the paracentesis.
And this patient had aperibulbar block, so the next step hereis to inject dispersive viscoelasticto fill the anterior chamber to the appropriate tension.
Here it's important to note thatthe appropriate tension is importantas a too soft eye willpredispose you to a long incision,and an over-inflated eye.It may create a short incision.And here I am stabilizing the eye with the0.12 clear Bs to the paracentesis, and with the2.5-mm keratome blade I am creating thetemporal main incision just anterior to the limbus.Here I'm creating atriplanar corneal incision,which is important in creating a watertight incision.
CHAPTER 3
And here, we are initiatingthe capsulotomy with the cystotome.I like to place the cystotomeon a cohesive viscolastic.This allows me if I encounter any trouble withthe capsule running out or notturning in the direction I like-with the cystotome, I can immediatelyinject the cohesive viscoelastic to try toaid in redirecting the capsulotomy.
Here Utrata forcepsare then used topropagate the initial capsulotomy with\Na continuous curvilinear capsulorhexis.And here as we create thecontinuous curvilinear capsulorhexis,I like to shoot typicallyfor approximately 5-mm capsulotomy,and this givesexcellent overlap of the lens optic,which is appropriately 6 mm.
So following completion of the capsulotomy,we mobilize the lens nucleus with hydrodissection.I like to use a flat cannulafor hydrodissection.It propagates a nice fluid wave.Here, we've also-hydrodeliniated the lensas you can see withthe golden ring sign here.And-following hydrodissection, we ensure good mobilizationof the lens by turningthe lens nucleus in both clockwiseand counterclockwise direction.
Once we've demonstratedgood mobility and rotation of the lens,anterior with the phacoemulsification handpiece-here, we're initiating the initial groovein order to split the nucleus into 2 halves.I'm using a Grayson\Nas my second instrument.And we'replacing both the Grayson andthe phacoemulsification handpiece deepinto the base of the groove.Following the initial crack, I move on togroove the first heminucleus,and again, crack it into quadrants.And this process is repeatedfor the second heminucleus.Aftercreating 4 quadrants,we switch to the quadrant removalsetting on the phacoemulsification machine,and...We bring the initial quadrantforward into the iris plane.There I was unable topurchase the first piece,but we were able to debulk it somewhat,and moving on to the second piece,we were able to elevate it up into the iris plane.We elected to move forward to the second piece asmost of the central nucleusI haven't aspirated,and I don't like toreach too far out into the peripherywith a phacoemulsification handpiece.Any surge orinstability can create capsular rupture.So again, you can notice thatthroughout quadrant removal,the second instrument, the Grayson,has been useful to help mobilize andessentially feedthe phacoemulsification handpiece.And here we have the last quadrant,and it's important to be careful at this stagewith the last quadrant as theposterior capsule can be very floppy.And, with any post-occlusion surge,the posterior capsule can move anteriorly and-be popped by the phacoemulsification handpiece.As we were able to achievegood hydrodelineation in this case,epinuclear shell was then removedon the epinuclear setting onthe phacoemulsification machine.Now the nucleus and the epinucleus have beencleared from the capsular bag.
Irrigation-aspiration handpiece is introducedto remove the cortical remnants.I like to-go after the subincisional cortex firstas the residual cortex-filling the capsular bag tends tohelp hold the posterior capsule back.So, as you can see, I'm-\NI've turned the port down.You'll notice that I havequite long capsular tags.This is intentional as I didn'tdo any central cortical cleanup priorto initial phacoemulsification that helps meto facilitate cortical cleanup,especially with the subincisional cortex.So we slowly make our way around-clearing up the cortex 360 degrees.Now we inspectthe posterior capsule.We do see some lens epithelial cells\Npersisting on the posterior capsule.So I'm doing a little bitof mechanical polishingwith the irrigation-aspiration handpiece.And here I've-despite the mechanical rubbing,some of the lens epithelial cells persist,so I turn the port down.
I do attempt to polish, butthe posterior capsulecame up to the port a bit,so I elected to switch toa Nightingale capsular polisher.This is donewithout any viscoelastic,and this does a very nice jobof removing any central lens epithelial cells.
Following completion of capsular polish,I inject acohesive viscoelastic to fill the capsular bag.And this creates theappropriate amount of spacefor the injection of the lens implant.
Here I'm injecting a 1-piece acrylic intraocular lenswith a wound-assisted technique.And I like to inject the lens directly into the capsular bag.Here I'm using a Kuglen hook toensure that the lens and the haptics arecompletely in the capsular bag.And I use the Kuglen hookto center the lens properly.I like tokeep my lens haptics withthese 1-piece acrylic lenseswith the square edge at the3- and 9-o'clock positionsto try to limitany chance of negative dysphotopsia postoperatively.
Following centration of the IOL,automated irrigation-aspiration is usedto remove the remaining viscoelastic material.Here, I'm clearingthe anterior chamber of boththe cohesive and any leftover dispersiveviscoelastic.I'm tilting and tapping the IOLto removeor capture any of the viscoelastic thatmight be trapped behind the intraocular lens.I also like to sweep the anglesfor any dispersive viscoelastic.
CHAPTER 4
Now, the case is completed.I am forming the anterior chamberand hydrating the temporal corneal incision.A little hydration of the paracentesis as well.Checking the ocular tensions.It's a little soft, soI inject a little bit more balanced salt solution.
And then, checking the incisions with the Weck-Cel.I like to press on the posterior wound edge.Here we see a little bit ofan egress of BSS,so a little bit more stromal hydration.Again, checking the tension.And, again the Weck-Cel's to checkfor any leakage at the temporal wound.And a little bit of pressure.The wound appears dry.One last check of the tension.It was a little bit firm, soburp in the paracentesis to release a littlebit of balanced salt solution.One last check of the wound.Both the temporal incision and the paracentesisappear to be watertight.We remove the lid speculum.The drapes are removed,and then the eye is dressedwith an antibiotic/steroid ointment, and a soft patch, and hard shield.
CHAPTER 5
Hydrodissection in any phacoemulsification technique is very important.Good rotation of the lens nucleus is critical forlens manipulation and reducing zonular stress.It allows for better stability of the capsular lens complexand positioning of the implant,so it really decreases the risk of complications byhaving good hydrodissection.And after that, I think,you know, for this particular technique,a good deep central groove,I find, is more important thanhaving long grooves, so thethickest part of the lens is centrally.So here,a good deep central grooveis really critical to get through any denseposterior plates that might be in the nucleus,and we will allow good propagation of yournuclear cracking.The othertip that I would suggest isbefore the initial groove,instead of doing a little bit of cortical cleanup,to leave the cortical tags there after allthe nucleus is removed.Those long cortical tags really help tofacilitate cortical removal, especiallythe sub-incisional cortex.I'll be using a 1-piece acrylic lens.\NIt's the AMO Tecnis 1.I like to use itbecause of the ease of injection, and theway that it sits in the capsular bagis very nice.It has good optical quality and-a good stability, and the designwith the square edge is thought toreally minimize the risk of posterior capsule opacity.Phacoemulsification machinesare quite efficient.The fluidics are quite good.I'm sure that there will continue to besmall incremental changes in the efficiencyand the fluidics of the machines,but-phacoemulsification hassort of stabilize in its advancements in termsof the ultrasound technology itself.The improvements-I feel will be more related tothe fluidics and the stability of the fluidswithin the eye during the surgery.As far as,you know, what we have availablewhere the future lies in supplementsto the surgery to improve our outcomes,You know, there are severalthings that are available-several technologies that are already availablethat can help to improve our outcomesand the safety of our surgeries.Intraoperative aberrometry hasreally become an important toolin our ability to predict or improveupon the predictability of our refractive outcomes.This allows us to obtain real time dataafter the cataract has been removedto confirm the powerof our lens implants.And there are also- these aberrometerscan also help us to align anyastigmatic correctionthat we're planning to use as well.Additionally, femtosecond lasers have beenincorporated into cataract surgery as well, again,to try to improve uponthe safety profile of already an extremelysafe procedure by improving the reproducibilityof the capsulotomy as well asdecreasing the use of ultrasound bypresoftening the lens nucleus.Patients are typically on topical medicationsfor approximately 1 month.These include an antibiotic drop,a topical nonsteroidal,and a topical steroid.Most patients will have some limited physical activity-no heavy lifting or straining.Generally, I tell my patients not to lift anythingmore than 5 or 10 pounds for at least the first week-first month would be preferable.We try not tohave them get any water in the eye,or, really critical is, that they don't rub their eyes during the procedures.And we have them wear a shield at nighttimefor the first week or two also,just when they're sleeping at night to try tolimit any-unintended trauma while they're sleeping at nighttime.