
Arthroscopic ACL Reconstruction with Bone Patellar Bone Graft using Anteromedial Technique
,
Boston University School of Medicine - Boston Medical Center
Main Text
Table of Contents
There are approximately 200,000 anterior cruciate ligament (ACL) injuries per year in the United States and more than half will be treated with ACL reconstruction. The diagnosis is made by physical exam supplemented by radiographs and MRI scan. Successful ACL reconstruction returns most athletes to pre-injury activity; however, outcome depends on appropriate preoperative evaluation, surgical timing, surgical technique, and an effective postoperative physical therapy program. Specifically, graft choice, graft positioning, and fixation technique have been shown to play important roles in patient outcome. Surgeons must also be aware of concomitant meniscal tears and cartilage injury that may need to be addressed at the time of ACL reconstruction. In the present case, we perform an anatomic ACL reconstruction with bone-patellar tendon-bone (BTB) autograft using an anteromedial drilling technique and flexible reamers for a young college athlete. The anteromedial approach offers the advantage of reliably reproducing the native anatomy of the ACL on the femur footprint by drilling the femoral tunnel independently of the tibial tunnel. Furthermore, using a flexible reamer instead of a straight rigid reamer allows for a longer femoral tunnel and lower risk of posterior wall blowout or fracture.
This is a 19-year-old collegiate intramural athlete that sustained a non-contact injury of his right knee while playing ultimate Frisbee. He described twisting on his right knee when he heard a “pop”. He had a large joint effusion when he was initially evaluated at a local emergency department. He presented to our orthopedic office approximately one month after his injury. At that time, he had minimal pain but felt the knee “buckle” on him several times per week. He was unable to return to his pre-injury level of participation as an active collegiate student involved in intramural athletics.
On exam, this patient had a moderate knee effusion and could flex his knee from 0 to 130 degrees. He had mild tenderness over the lateral joint line with slight opening of 5 degrees with valgus stress at 0 degrees but not at 30 degrees. His knee was stable to varus stress. He had a grade 2B Lachman test with a positive pivot shift. The dial test in the prone position at 30 and 90 degrees of knee flexion was symmetrical. He had normal sensation and blood flow to the lower extremity.
Initial imaging consists of a knee trauma radiograph series including anteroposterior, lateral and patellar views.1 The images should be closely reviewed for bony avulsion fractures and any associated bony injuries. The Segond sign (small avulsion off the lateral tibial plateau) represents a lateral capsular avulsion which should raise suspicion for an ACL rupture.2 In select patients at risk for knee osteoarthritis, posterior to anterior, 45 degree flexion weight-bearing films may be obtained.3 Knee MRI is the most sensitive and specific in diagnosing ACL injuries. Bone contusions of the lateral femoral condyle and posterior tibial plateau are the most common associated finding.4 Injuries to the menisci, collateral ligaments and posterior cruciate ligament are also reliably detected on MRI. Knowledge of concomitant knee injuries is essential for preoperative planning.
This patient has recurrent episodes of symptomatic knee instability following his initial injury. The medial collateral ligament and menisci are often injured at the time of initial injury with lateral meniscus injuries more common acutely. Untreated ACL injuries may lead to further chondral and meniscal injuries. It is unclear if ACL reconstruction will reduce the incidence of arthritis.5, 6
Treatment options include physical therapy starting with an emphasis on reestablishing full range of motion (flexion and extension) and controlling the effusion followed by quadriceps and hamstring strengthening. Then, a sport-specific rehabilitation protocol may be initiated. For high demand athletes and active patients with symptoms of instability, surgical ACL reconstruction is recommended. Both open and arthroscopic techniques exist with multiple graft choices including autograft (BTB, quadrupled hamstring, quadriceps tendon) and allograft (semitendinosis, Achilles tendon, BTB, tibialis anterior, tibialis posterior).
Compared to open surgery, arthroscopic ACL reconstruction is associated with a shorter recovery and rehabilitation time with a decreased risk of infection. Partial meniscectomy, meniscal repair, and procedures for cartilage damage can be performed simultaneously. Autograft tissue is associated with a decreased re-rupture rate in young athletes when compared to allograft tissue.7 ACL reconstruction with BTB autografts have similar clinical outcomes when compared to the use of hamstring autografts. However, recent clinic studies have shown decreased failure rate with BTB autograft and a more stable knee on KT 1000 testing.8 Furthermore, the anteromedial approach for ACL reconstruction offers the advantage of reliably reproducing the native anatomy of the ACL femoral footprint by drilling the femoral tunnel independently of the tibial tunnel. Historically, this has been challenging to accomplish with a transtibial technique. We propose that using a flexible reamer instead of a straight rigid reamer allows for a longer femoral tunnel and lower risk of posterior wall blowout or fracture.
- AcuFex Anatomic ACL Instrumentation by Smith and Nephew, Andover, MA
- Stryker Flexible ACL Versitomic drills
- Stryker Metal Interference screws.
Absolute contraindications to arthroscopic ACL reconstruction include any patient with an active knee infection or who is unfit for anesthesia. Relative contraindications include patients who are unlikely to follow post-operative rehabilitation protocols. Failure to comply with rehabilitation may result in arthrofibrosis and a poor outcome. Relative contraindications to patellar tendon harvest include patients who have preexisting anterior knee pain, jobs that require kneeling (Clergy, carpenters), jumping sport athletes, older patients, and those with narrow patellar tendons or patellar chondrosis.
At 4 months post-operatively, our patient has pain free range of motion from 0 to 130 degrees of knee flexion with a grade 1A Lachman test, a negative pivot shift, and no varus or valgus instability.
Pre-operative radiographs shows slight anterior translation of the tibia in relation to the femur on the lateral image.


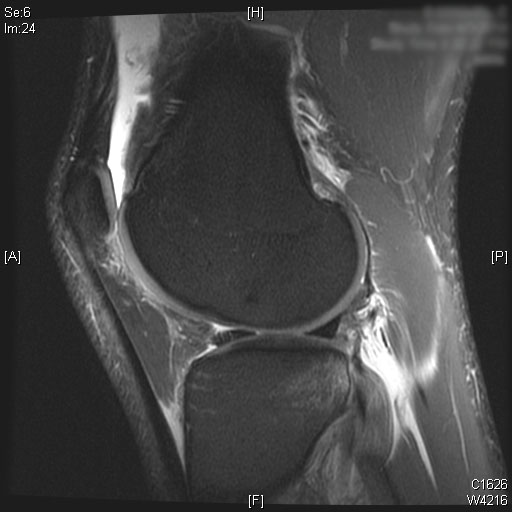
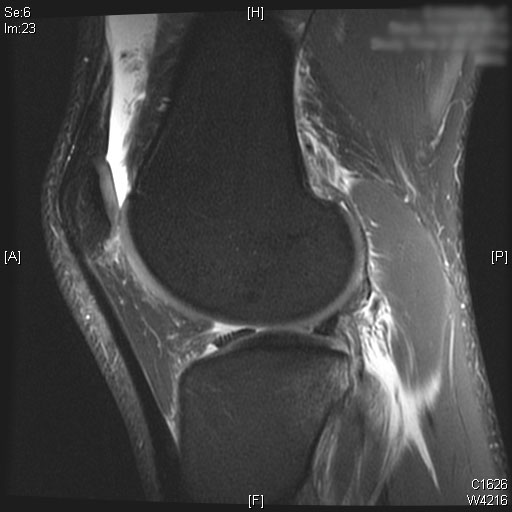
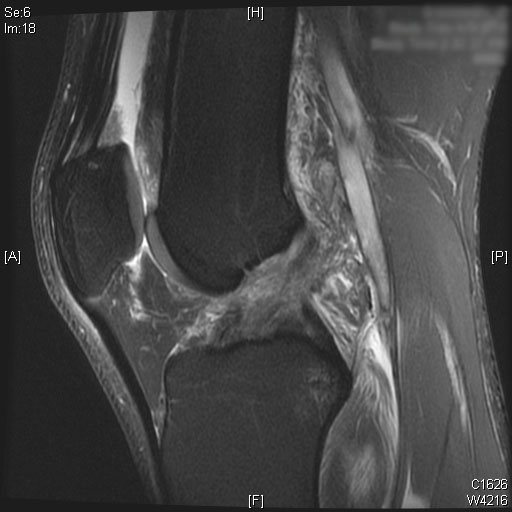
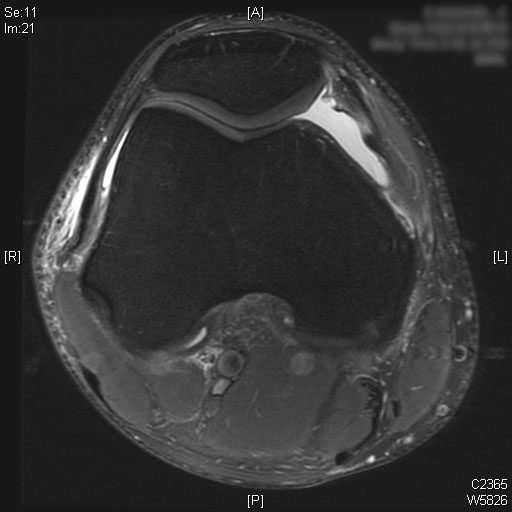
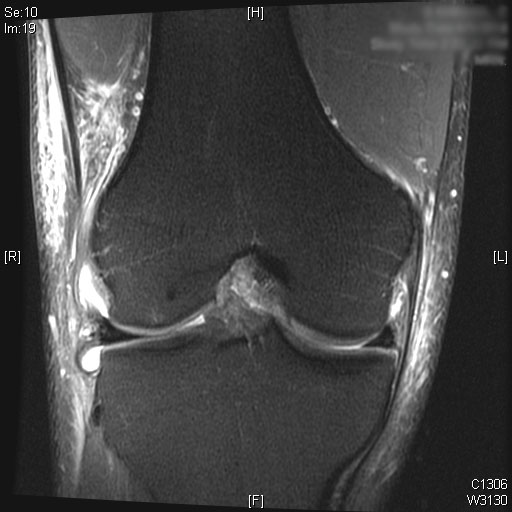
Complete ACL rupture is seen on the sagittal T2 MRI images. Also, bone marrow edema is seen on the posterior third of the lateral tibial plateau. Cartilage on the medial and lateral femoral condyle alone with the patella is preserved. Moderate joint effusion is visualized on the T2 MRI images.




ACL reconstruction for ACL ruptures is associated with a high rate of return to sports performance and improved knee functional scores.9 In patients who wish to return to sports, reconstructing the ACL has been shown to reduce the rate of further osteochondral and meniscal injury.5, 6
Femoral tunnel placement has been an issue of debate with many published studies. Recent literature suggests that a lower lateral tunnel in the 10:30 or 1:30 position will more accurately recreate the position and function of the natural ACL, especially the rotational stability. This anatomic femoral tunnel position can be achieved with the use of an anteromedial portal and straight reamers, flexible reamers, and even the transtibial technique with hyperflexion of the knee.10 Historically, traditional transtibial ACL reconstruction techniques resulting in a vertical ACL graft have been associated with improved knee stability in the anterior to posterior plane, but with persistence of rotational instability and a positive pivot shift.8, 11 Biomechanically, double bundle ACL reconstruction where both the anteromedial and posterolateral bundles are reconstructed will most closely reproduce natural ACL function. However, Adachi et al. failed to show any clinical difference between a single bundle and double bundle technique in a prospective randomized controlled trial of 108 patients.12 Until a clear clinical benefit for double bundle anatomic ACL reconstruction is demonstrated, we prefer a single bundle anatomic technique that is achieved by using an anteromedial portal and flexible reamers for femoral tunnel drilling.
Altentorn-Geli et al. compared the clinical outcome data of patients after ACL reconstruction using a transtibial (TT) technique compared to an anteromedial (AM) technique. The authors reported significantly faster recovery time from surgery, walking without crutches, and return to normal life with the AM technique. In addition, patients in the AM ACL reconstruction group had significantly better knee stability (KT-1000, pivot-shift test, Lachman test, and IKDC scores) compared to the TT group. Koutras et al. also showed better Lysholm knee scores and performance in patients after AM ACL reconstruction compared to a TT technique with short-term follow-up.13 Furthermore, Mardani-Kivi et al. also reported significantly faster return to activity, better range of motion, and greater patient satisfaction in the AM ACL reconstruction group. However, he did not show a difference in Lachman testing or knee stability.14
In addition, the use of an autograft construct has been shown to have a decreased rate of re-rupture in young active athletes compared to allograft.7 We reserve allografts for older (> 40 years of age), low demand patients or for revision cases where autograft choices may be limited. Patellar tendon grafts have less laxity (KT-1000) compared to hamstring grafts and some studies have also demonstrated lower failure rates.15 However, BTB grafts are associated with slightly higher rates of anterior knee pain.
- Obtain a medical history including the mechanism of injury, previous injuries, type of sport and activity level
- When and how did the injury occur? What was the mechanism?
- What symptoms do you currently experience? Is there pain or instability? What limitations in activity have occurred as a result of injury?
- What prior treatments has the patient tried (physical therapy, activity modification, medications)?
- Visually inspect the knee for an effusion, ecchymosis, and the condition of the skin.
- Carefully palpate the knee joint. Joint line tenderness may indicate a meniscus injury. Any defect in the extensor mechanisms or extensor lag may be indicative of an extensor mechanism injury.
- Evaluate active and passive knee range of motion. Any loss of passive extension may be due to a displaced bucket handle meniscus tear or arthrofibrosis. Loss of flexion may result from significant knee effusion.
- The knee should be stressed with a varus and valgus force at 0 and 30 degrees of flexion to detect collateral ligament injuries. Any instability at 0 degrees correlates with a collateral ligament injury with rupture of one or both cruciate ligaments.
- Injuries to the posterior cruciate ligament and posterolateral corner should be tested for with the posterior drawer test and the external rotation dial test in the prone position, respectively.
- Patellar instability can also be assessed with apprehension testing by applying a laterally direct force on the patella with the leg in 20 to 30 degrees of flexion. In this position, the patella is engaged in the trochlea groove.
- Tests for anterior cruciate ligament (ACL) rupture
- The Lachman test is performed with the knee flexed 20 to 30 degrees with one hand stabilizing the femur. The other hand is then used to apply an anterior force on the tibia from a neutral starting position. Laxity is compared to the contralateral side. The test can be graded according to the degree of anterior displacement.1 Grade 1 is up to 5mm difference, Grade 2 is 5 to 10mm, and Grade 3 is > 10mm of anterior translation. The letter ‘A’ is applied after the grade if a firm endpoint is present with anterior translation while the letter ‘B’ is applied if there is no firm endpoint.
- The Pivot shift test can be used to assess the degree of rotational knee dysfunction. It is difficult to perform clinically, but is very sensitive during examination under anesthesia.2, 3 With the patient supine, the affected leg is slightly abducted to relax the iliotibial band. Then, an internal rotation and valgus force is applied while the examiner passively flexes the knee. In an ACL deficient patient, a positive pivot shift is typically detected from 20 to 40 degrees of flexion, which is when the anterior subluxated tibia is reduced by the iliotibial band.
- In the ACL deficient knee, the knee will subluxate anteriorly between 20 and 40 degrees of flexion. A positive pivot shift test is typically detected between 20 and 40 degrees of flexion, which is when the anterior subluxated tibia is reduced by the iliotibial band.
Outcomes for ACL reconstruction are favorable with success rates of up to 95%. In a retrospective review of 97 patients by Bach et al., 70% of patients had less than 3-mm on KT-1000 arthrometer testing. The same group also reported significant improvements in Teneger activity level, a mean Lysholm score of 87, and good to excellent modified Hospital for Special Surgery scores for 82% of patients.13 A review of recent literature by Chalmers of studies with more than 10 years of follow-up compared cohorts of 685 patients treated nonoperatively and 1585 patients treated with ACL reconstruction. The operative group had significantly improved activity levels according to the Tegner score, fewer subsequent meniscal injuries, and significantly fewer additional knee operations. However, they did not identify any difference in the Lysholm score, the IKDC score or the development of radiographically evident osteoarthritis.14
In active patents with an ACL tear, early ACL reconstruction may be more cost effective than delayed treatment after physical therapy. Mather et al. used the Multicenter Orthopaedic Outcomes Network (MOON) database to show that early ACL reconstruction was more effective in improved quality-adjusted life-years gained at a lower cost compared to optional delayed reconstruction after a period of rehabilitation.15
With increasing numbers of young at risk athletes, future research is turning to injury prevention. Multiple recent studies have noted the ability of injury prevention and neuromuscular training to reduce the incidence of ACL ruptures. Cost-effectiveness studies Sadoghi et al. and Swart et al. demonstrated that universal neuromuscular training is the most cost effective method of ACL injury prevention.16, 17
The author has no financial relationship with any of the companies mentioned in this article.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Torg JS, Conrad W, Kalen V. Clinical diagnosis of anterior cruciate ligament instability in the athlete. Am J Sports Med. 1976;4(2):84-93. doi:10.1177%2F036354657600400206.
- Fetto JF, Marshall JL. Injury to the anterior cruciate ligament producing the pivot-shift sign. J Bone Joint Surg Am. 1979;61(5):710-714. doi:10.2106/00004623-197961050-00010.
- Bach BR Jr, Warren RF, Wickiewicz TL. The pivot shift phenomenon: results and description of a modified clinical test for anterior cruciate ligament insufficiency. Am J Sports Med. 1988;16(6):571-576. doi:10.1177%2F036354658801600603.
- Yoon KH, Yoo JH, Kim KI. Bone contusion and associated meniscal and medial collateral ligament injury in patients with anterior cruciate ligament rupture. J Bone Joint Surg Am. 2011;93(16):1510-1518. doi:10.2106/JBJS.J.01320.
- Fithian DC, Paxton EW, Stone ML, et al. Prospective trial of a treatment algorithm for the management of the anterior cruciate ligament-injured knee. Am J Sports Med. 2005;33(3):335-346. doi:10.1177/0363546504269590.
- Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR. Fate of the ACL-injured patient: a prospective outcome study. Am J Sports Med. 1994;22(5):632-644. doi:10.1177%2F036354659402200511.
- Pallis M, Svoboda SJ, Cameron KL, Owens BD. Survival comparison of allograft and autograft anterior cruciate ligament reconstruction at the United States Military Academy. Am J Sports Med. 2012;40(6):1242-1246. doi:10.1177/0363546512443945.
- Spindler KP, Huston LJ, Wright RW, et al. The prognosis and predictors of sports function and activity at minimum 6 years after anterior cruciate ligament reconstruction: a population cohort study. Am J Sports Med. 2011;39(2):348-359. doi:10.1177/0363546510383481.
- Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o'clock and 10 o'clock femoral tunnel placement. Arthroscopy. 2003;19(3):297-304. doi:10.1053/jars.2003.50084.
- Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon: a cadaveric study comparing anterior tibial and rotational loads. J Bone Joint Surg Am. 2002;84(6):907-914. doi:10.2106/00004623-200206000-00003.
- Musahl V, Plakseychuk A, VanScyoc A, et al. Varying femoral tunnels between the anatomical footprint and isometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med. 2005;33(5):712-718. doi:10.1177/0363546504271747.
- Adachi N, Ochi M, Uchio Y, Iwasa J, Kuriwaka M, Ito Y. Reconstruction of the anterior cruciate ligament. Single- versus double-bundle multistranded hamstring tendons. J Bone Joint Surg Br. 2004;86(4):515-520. doi:10.1302/0301-620X.86B4.14856.
- Bach BR Jr, Tradonsky S, Bojchuk J, Levy ME, Bush-Joseph CA, Khan NH. Arthroscopically assisted anterior cruciate ligament reconstruction using patellar tendon autograft. Am J Sports Med. 1998;26(1):20-29. doi:10.1177/03635465980260012101.
- Chalmers PN, Mall NA, Moric M, et al. Does ACL reconstruction alter natural history?: A systematic literature review of long-term outcomes. JBJS. 2014;96(4):292-300. doi: 10.2106/JBJS.L.01713
- Mather III RC, Hettrich CM, Dunn WR, et al. Cost-effectiveness analysis of early reconstruction versus rehabilitation and delayed reconstruction for anterior cruciate ligament tears. Am J Sports Med. 2014;42(7):1583-91. doi.org/10.1177/0363546514530866
- Sadoghi P, von Keudell A, Vavken P. Effectiveness of anterior cruciate ligament injury prevention training programs. J Bone Joint Surg Am. 2012;94(9):769-776. doi: 10.2106/JBJS.K.00467
- Swart E, Redler L, Fabricant PD, Mandelbaum BR, Ahmad CS, Wang YC. Prevention and screening programs for anterior cruciate ligament injuries in young athletes: a cost-effectiveness analysis. J Bone Joint Surg Am. 2014;96(9):705-711. doi:10.2106/JBJS.M.00560.
Cite this article
Nathan D. Orvets, MD, Xinning "Tiger" Li, MD. Arthroscopic acl reconstruction with bone patellar bone graft using anteromedial technique. J Med Insight. 2016;2016(45). https://doi.org/10.24296/jomi/45Procedure Outline
Table of Contents
- General endotrachial anesthesia. (Sedation and Spinal is another option)
- No femoral block for ACL reconstruction due to quadriceps inhibition in the postoperative period.
- Range of Motion, Varus/Valgus Stress, Lachman and Pivot Shift Test
- Before beginning surgery, an examination under anesthesia is performed. It is essential to evaluate ROM, Lachman test and Pivot Shift before starting surgery or graft harvest.
- Compare to Contralateral Leg
- Patient is positioned supine on a regular operating room table with a post on the ipsilateral mid thigh.
- A tourniquet is applied snugly as far proximal on the thigh as feasible.
- After skin preparation and draping, a 5 to 7 cm midline knee incision centered over the patellar tendon is marked with a skin marker (BTB can also be harvested with horizontal incision).
- The limb is exsanguinated and the tourniquet inflated to 250 mmHG.
- Anatomic Landmarks
- A 5 to 7 cm midline incision is made over the patellar tendon with a #15 scalpel.
- Skin Incision and Dissection Down to Patellar Tendon
- Dissection is carried down to the paratenon which is carefully reflected off the underlying tendon and preserved for repair. (Use a #15 scalpel to dissect the paratenon).
- Mark and Measure Graft
- Cut Graft
- Using a #10 scalpel, 10 mm central third patellar tendon is harvested extending from the patella to the tibial tuberosity with the knee in flexion, and then dissection is completed with the knee in extension.
- Saw to Remove Graft
- A 10x25 mm bone block is taken from both the patella and the tibia using a micro oscillating saw taking care not to cut deeper than 15 mm so as to prevent an iatrogenic fracture.
- Use Osteotome and Mallet
- Use Metzenbaum Scissors to Remove Graft
- Femoral Graft Cuts with Saw
- Use Osteotome to Free Graft
- Measure
- Bone blocks are carefully removed with a curved osteotome.
- Trim and Sequentially Size Femoral Side
- The graft diameter is carefully measured on the back table. Bone block is shaped with a ronguer to fit through a 10 mm tunnel for the femur and 10.5 mm tunnel for the tibia.
- It is important that the bone plug goes through the 10 mm sizer easily to allow passage of the graft.
- The plug is shaped to match a bullet for the femoral side to further allow turning of the graft to go into the femoral tunnel with ease.
- Trim and Sequentially Size Tibial Side
- The bone block is placed in Bacitracin solution for 10 mins.
- Diagnostic Arthroscopy
- An anterolateral portal is established with the assistance of an 18 gauge spinal needle using an outside-in technique. The portal is just above the meniscus and it is essential to check the trajectory of the needle and make sure it is directed to the footprint of the ACL on the femoral side.
- An anteromedial portal is then established with an #11 blade, and capsulotomy is performed cutting from an inferior to superior direction with the blade facing up. It is positioned just above the medial meniscus to allow adequate visualization of the femoral ACL footprint.
- A thorough diagnostic arthroscopy is performed closely examining the patellofemoral, medial and lateral compartments.
- Any meniscal pathology is addressed with either repair or partial menisectomy depending on the tear type and location.
- The torn ACL remnant is debrided with ArthroCare device and shaver. A small notchplasty is done to allow improved visualization.
- Alternatively, the senior author prefers the trans-notch portal through the patella tendon harvest site. This viewing portal allows excellent visualization of the ACL footprint for drilling.
- Notchplasty
- A small notchplasty is performed with a high-speed burr until adequate visualization of the femoral footprint is established. An aggressive notchplasty is not critical as long as the tunnel positions are easily identifiable and there is no graft impingement in full extension.
- Use Arthroscopic Awl
- The back wall of the femur is identified after debridement of the soft tissue. The anatomic position for ACL on the femoral side is located at the 10 to 10:30 position for a right knee (1 to 1:30 position for a left knee).
- Use Guide and Drill Tunnel
- A femoral tunnel over the top guide is used to help retain 1 to 2 mm of posterior wall following drilling. If drilling a 10 mm tunnel, a 6 or 7 mm offset guide should be used. The senior author prefers a 2 mm back wall. (7 mm over the top guide)
- Flexible Reamer
- The femoral tunnel is drilled through the anteromedial portal with the use of a flexible reamer (Stryker Versitomic Reamers) to match the width and depth as the bone block (10 mm diameter and 25 mm depth in this case). The senior author prefers to make the bone plug for the femoral side to measure 9.5 mm in diameter and 23 mm in length to allow ease of passage.
- Pass Suture Through Tunnel
- A #2 fiberwire is shuttled through the femoral tunnel to help assist in graft passage.
- Use Tibial Guide on Plateau
- Setting of the tibial guide is dependent on the length of the patella tendon. The rule is add 10 degrees to the patella tendon length. Typically, the tibial guide is set at 55 to 60 degrees.
- Drill Tibial Tunnel
- A tibial tunnel drill guide is positioned such that the tunnel is located at the center of the native ACL footprint. This should also be adjacent to the slope of the medial eminence and along a line extended from the posterior border of the anterior horn of the lateral meniscus.
- The obliquity of the ACL is restored when the guide pin is slightly on the medial tibial eminence.
- The guide wire is placed and the tunnel is drilled with a 10.5 mm diameter drill bit.
- Ream Tunnel
- Clear Tunnel of Soft Tissue
- Soft tissue from both tunnels is cleared with the ArthroCare.
- Final Graft Preparations
- Graft Inserted
- Shuttle sutures are placed through both bone plugs and the graft is passed into the tibial tunnel and then to the femoral tunnel.
- A needle driver or grasper maybe used to help turn the graft on the femoral side if difficulty is encountered
- Femoral Interference Screw
- An interference screw is placed in the tibial tunnel after tensioning is complete, and the knee is placed in 20 degree flexion. The senior author prefers to use a 8 mm x 25 mm screw if the tunnel is drilled to 10.5 mm in diameter.
- Assess Knee
- Cycle Knee to Tension Graft
- The graft is tensioned by repetitively cycling the knee through a complete range of motion (20 cycles).
- Fixation of Tibial Side with Interference Screw
- An interference screw is used to fix the femoral side superior to the graft. The senior author prefers to use a 7 mm x 20 mm screw if the tunnel is drilled 10 mm x 25 mm in size.
- Check for Impingement
- Knee is evaluated one more time with the Lachman test to assess for graft stability.
- The paratenon is carefully closed with buried #0 vicryl suture. In addition, the patella tendon is also closed with interrupted #0 vicryl sutures in a buried fashion.
- Place previously collected bone graft in the patellar defect.
- Skin is closed with running 3-0 monocryl with Steri-Strips.
- A dry sterile dressing and ice therapy device is applied, and knee brace locked in extension are applied before leaving the operating room.
- Partial weight bearing in a hinged knee brace locked in extension for 4 weeks.
- Brace is opened 0 to 90 from 4 weeks to 6 weeks and completely opened after 6 weeks.
- Patient may transition to a smaller post operative knee brace at 8 weeks after surgery (Road runner ACL brace).
- Post operative follow-up visits are normally scheduled at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year after surgery.
- Range of motion and physical therapy are typically started 2 weeks post-operatively.
- Patients may begin jogging at 3 to 4 months depending on progress and may resume sports between 6 months to 9 months depending on the type of sport and also when full quadriceps strength returns.
Transcription
CHAPTER 1
Alright, so this is a 19-year-old gentleman who was playing ultimate frisbee in college, had a pivot shift event, and he heard a pop in his knee. He came in with some instability and with MRI demonstrating ACL tears. You can see the most important thing, the first thing you do, is you need to do an exam under anesthesia and it’s important to examine the knee here. Test for range of motion. You can see he has 140 degrees range of motion, zero deflexion, and good extension. And then now we do a Varus/Valgus stress. That’s done at 0 degrees, which is stable, and at 30 degrees here with a Valgus stress testing the MCL. And with the Varus stress here, it’s 0 degrees. Opens up just a little bit but that’s very symmetrical with him, in comparison to the contralateral side. And then here at 30 degrees.
Testing it for the ACL, the most sensitive test is the Lachman examination. It’s done at 20 to 25 degrees of flexion, right about here. You put one thumb here on the femur to stabilize it, here on the tibial tubercle, and then anterior translation. You can see he has no end point, and that’s pretty gross translation. I would call that either a 2b or 3b Lachman, depending on what the subjective value. I think it’s at least 15 mm in my exam. And here’s the pivot shift, you internally rotate the leg. Here put your hand right at the proximal tibia. With rotation you can see there’s quite a bit of pivot in this gentleman. You see that? So it’s grossly unstable here. You put the knee at 90 degrees. Feel for the condyle. Tibial plateau here is a centimeter in front. Negative posterior drawer therefore there’s no PCL injury in him.
It’s also very important to check the contralateral side. So here’s a normal side here. Same, very symmetrical range of motion. Here you can see Valgus stress does not open, and then you can see the Varus stress opens up a little bit which is very symmetrical to the other side. Lachman exam, 25 degrees or so, very stable. And then with a pivot shift here, you can see there is no pivot. And then he has a very symmetrical side over here. The tibia is about a centimeter in front of the femur, which is the normal position here.
Alright so setup for ACL. What I do is, you want to make sure, I break the bed down here. So here’s the region where the bed will break down. We move the patient down so the knee is past that region, and the entire bed breaks down. You can also do this with a leg holder, but I just typically like just to break the bed down to do the ACL. Here’s a post, I use a post here for all my knee surgeries here. Kind of right here at the mid-thigh and the patient goes all the way over a little bit so you can drop the leg down, and then you can use the post too for Valgus stress. So we’re going to move the patient down before we start the case.
Good? Ok, tourniquet up, please. Ok, alright.
CHAPTER 2
Alright, so the first step is going to be the bone-patellar-bone-harvest. I usually like to mark out the inferior pull of the patella here. Here’s the medial edge of the patellar tendon, right here. The lateral edge of the patellar tendon. Tibial plateau on the medial edge. Here’s the femoral condyle, plateau on the lateral side, and the femoral condyle here. So the first, for the ACL, the viewing portals. Typically what I use is like out here on the lateral side. High, so you can actually see down to the tibia for the footprint we do in the drilling. And then you want to be closer to the patellar tendon, so you can actually go around it and see the femoral wall when you do the femoral socket.
If you’re going to do a meniscectomy, the best portal is actually here in the soft spot, so you can actually see over here to the medial side. The anteromedial portal we do it under spinal needle guidance. And for the tibial tunnel, typically you feel for the plateau. There’s a spot between the metaphyseal and diaphyseal flare, and you come down and there’s actually a soft spot right here where the flare is. And the tibial tubercle is right here, and I typically like to go about 2 centimeters over. The reason for that is you want to be able to drill your tunnel and recreate the obliquity of the ACL graft. So it’s something like that. You don’t want to be this way on a tibial tunnel, so that’s why I like it to be about 2 centimeters over on this side. For this guy, he’s 6 foot 3 inches tall, so he’s going to have a bigger patellar tendon. So, I want to drop my hand and actually get the tunnel down a little bit distal so we don’t have a graft mismatch. So he’s probably going to be somewhere around in this region down here, his tunnel positioning.
I like to make a central incision just over the harvest site here. I used to make an incision on the medial side which goes all the way down, and you try to get both, tibial tunnel as well as the harvest, at the same time, but I feel that’s a little bit harder because you’re going to have to stretch the incision over to harvest. And then you’re going to have to go down to this position here, which makes it really hard and you have to extend the incision. So now I do two independent incisions, one centered over the BTB and the second one centered over the tunnel so you can have more play with the tunnel on this position. And you can see the skin actually stretches quite a bit up top, so you don’t have to make the incision so much higher on top, just at the edge of the patellar tendon. Here you can stretch it over, but when you go distal the incision doesn’t stretch as much, so you’re going to actually have to go down to the tubercle and actually extend the incision.
Okay, we’re just gonna do it here, watch out a second. Okay, go ahead. Okay and then you go ahead and just lift. And you just take a kind of feathering technique to go down into the patella here. You can see here’s some fatty tissue right around it. You can use all the incision here. Get rid of the soft tissue here, and then here’s the peritenon. Why don’t you go here. Okay so I’ve made an incision in the peritenon, as you can see. Now what I do is I take a, let me get a pickup, please. Can I have an Adson’s, please? So you can see here the medial side of the patellar tendon right here, and then the lateral aspect of the patellar tendon is right there. And you make a little incision to incise the peritenon. You pick that up, go extend it up, and you can see if you use a number 15 blade here, it dissects really nicely to get at the peritenon around the patellar tendon. It’s very thin for this gentleman here, and you like to try to repair theirs at the end if you can. So with the blade up you can just take that up. Okay, and come down here for me. Good. Can I have a pair of Metz please?
As you can see here in the patella, you just basically take this pair of Metz, you go underneath, you spread your Metz like that, and then you kind of come down and that opens up the tendon for you. And now you can actually make an incision to go and break down the tendon, the peritenon around the patellar tendon, superiorly around the patella. And you can see there’s a couple vessels here.
So you can see, here’s the patellar tendon, here’s the- I’m just going to put you right here. Medial edge right here, and then a lateral edge. And for this gentleman here, he is exactly 31 millimeters in width. So I like to take the central third, so you can actually mark this out if you want. So here’s the part here. Ten centimeters is the central third. You can do this freehand, you can do this with a double blade. Couple companies actually make a double blade that you can use-it’s safer, but. You take a 10 blade, a little bit bigger, a little bit longer length. You go down along the fibers, you cut down along the fibers all the way down to the bottom. If you can follow me here. Okay, good, perfect. Okay, and then come back up. So here’s the central third right there, and this one I’m going to cheat just a little bit lateral to my lateral line over here to make it a little of a nice bigger tendon for him here. Coming down here. Okay perfect.
So now we’re going to have the knee in extension, and then we’re going to go ahead and have two stents. So you can see, I got two retractors on my harvest site. Now I can identify where I am down below on the tubercle and just extend the incision down over here. Okay, and then I move over and do the same thing on this side. And then this is going to go over here, and you’re going to hold down here for me. Can you hold this right here? Now I’m going to extend this down, just kind of in line, and that’s about 10 millimeters in width. And then you typically, you could measure this, but if you eyeball it, I like the 25 millimeters in length and this is going to be on my femoral side. I typically flip the tibial to be the femoral side. And usually if you want you can measure this, but if you’ve done this enough times you don’t really need to. Exactly 10, you can see there. And then if I measure here from the top, to the bottom, it’s going to be just at 25, and you can see the top is right there. So this is about 25, so that’s a perfect sized plug.
Okay, grab here for me? Oscillating saw here, sagittal saw, 10 millimeters by about 25 length. You’re going to want to be kind of scorching here. You don’t have to bevel as much here. I do a little bit just so I take less bone, but on the patellar side you have to bevel. Okay, good. Okay now do the distal cut, which is going to be right about here. Okay, lap please? So you go over the corners again over here. Okay, and do the same thing on this corner. Okay, once you do that, you take a curved osteotome like this, you go to the top of the tendon where the-where this insertion point is here. Mallet. And then you tap down, and then it comes right out for you. Very easy, just like that. You take a pair of Metz, underneath, over here. Alright you guys can relax here, we’re going to go up top.
You can see, here’s a nice bone plug here. It’s harvested from the bottom. So I put this in a lap. Okay, good. Knife, please? Okay and now I’m going to extend this up. This is kind of on a fat pad. To go up against the tibia-patella here. So there’s the top. And then I’m going to have you just come down here, and have you come up here. Okay, so now this is the edge of the patella. So I’m going to go up like this. Alright, release this here Just a little over 10 and the length here at the bottom of the patellar tendon there is about, just about 25 as well. Okay, we’ll go ahead and have you, can you hold this right here for me? Okay good.
Okay so now, I’m right at the central third of the patella, so she’s going to hold this for me like that. Good. Perfect. So now the first step is you’re going to scorch this. Okay, once you scorch it, you want to drop your hand about 45 degrees, so you don’t go into the articular surface. Okay, that’s the medial side, now we go on the lateral side. This side here, perfect. And then we want to drop 45 degrees this way.
Do you have a pair of nail scissors? Okay, that’s good. Actually, that’s pretty good. And this is going to be our patellar side/tibial side, and I flip this, and you can see over here the patella does not violate the cartilage surface right here. And you actually have this nice 45 degree inclination down from this side and then this side, so that you don’t go down to the cartilage surface. Alright, so we’re going to prep the graft right now.
CHAPTER 3
So I’m just cleaning some of this fat pad off the graft here. I like to use the tibia side for the femur side. So this is going to be my femur side, and this is going to be my tibia side. And I mark off the graft here, so I can actually see where it is right there. So we measure this graft. It comes out to be just about 45 for this gentleman. He’s 6’3”. This is 45. This is actually a pretty short patellar tendon. It’s actually normal, but for him it’s a little bit on the shorter side. And what I do is I add 10 to that to set my degrees for my-for my guide, which is going to be about 55 degrees. And that will ensure you that you don’t have a graft-tunnel mismatch.
So now we start here, we’re going to use a number 11 tissue crumpler right here. I start with number 11 and we’re just going to crumple up this graft here. Pretty good bone. Okay, good. And then I take this, kind of get rid of this soft side here. Do you have a pair of like nail scissors? Okay so after 11, I go to a 10. So you kind of crumple it down a little bit there. Ensure a nice bone plug. Okay, so I measure the length of the bone plug here. It’s 30, so it’s a little bit long. I’m going to make it, I like to make this about 23 and I drill a 25 femoral tunnel. I think it’s important, just a little bit shorter, so it can turn that corner.
So right now it’s about a 27 still, so I’m going to just trim it down a little bit more. It’s important to bullet this. Actually, make this top a bullet shape, so that I can have it pass the corner without having any trouble. So like that. And then here you can see I usually use a, I do a 10 millimeter tunnel on my femur side, it’s still a little bit tight. And I find that it’s much easier when you make this 1 millimeter smaller than a tunnel to pass, so I go to a 9. Nice plug here, and it goes into 10. You can see here it goes into 10 very easily, so that’s what I’m going to do. I’m going to drill a 10 on my femur side. That’s going to be good.
Okay so now on the tibia side, same thing. Do you have a little basin? I’m going to put this bone in there so we can fill up the patella. And I check with a 10, still pretty tight. So I’m going to go to a 9. And I usually drill my tibial tunnel about .5 millimeters bigger than the femoral tunnel. So if I do a 10 then I’m going to do a 10.5 on the tibia side, just so that the plug can pass easily across the tibia into the femur. And this side you don’t need to bullet it because it’s going to be on my tibia side. You don’t need to pass the corner. I only bullet the femur side because the way it is, when you pass that corner, you have to turn it, and the longer it is the harder it is to turn that corner. Okay. So last time there. So you can see now, you can see the 10 goes through pretty easily. A little bit more snugger on that side, but that’s pretty good.
And then my top sides of my graft here is a 25 or 26 for the tibia side, and about 20-yea about 20- 24 or so for the femur side. And now I’m going to drill two sutures across. Do you have the drill, please? Here’s a 1.5 millimeter, this is going to be right at the tip here. It’s going to be just at the side. And the same thing on our distal side here. Okay. There you go. Alright, so let me get the sutures, I’ll get the orthocord first, and then the fiberwire after that. Okay, so I use two different sutures just to help me identify which one I’m going to pass. So for my femur side, I typically use the orthocord or something different than my tibia side. You can see it’s pretty easy to pass through here. Okay, let me get the other orthocord over here. Okay, cut for me. Thanks. So here’s the two orthocord, a little bit different colors, and then I’m going to pass the fiberwire number 2 on the side where I’m going to put it through my tibia. So, let me see the 2 fiberwire. Okay, so there is going to be a fiberwire here, and cut.
Okay, so this is our graft right here. Let’s take a look. The total length of the graft is 92 and the intra-articular portion for the patellar tendon is 45. You can see this is going to be my femur side right here. You can there’s see right here I bulleted the top, if you can take a look. So this looks like a bullet, right here. The reason you bullet is you can turn the corner much easier when you do that. And then on the tibia side you don’t have to do that as much, you can see it’s actually a more rectangular-shaped bone block.
And you double check this again, you want to make sure that it goes through a 9 point, a 10 very easily here, and this is going to go through a 10 pretty easily. A little more snug than the other side, but I do drill a 10 millimeter tunnel for the femur side and I do a 10.5 for the tibia. What I do is I soak in solution, this graft in the bacitracin solution for 5 minutes and then I take it out and put it in the gauze because I think it’s important, sometimes you may get a little bit of contamination, or just from the back table. So can you just take that out in 5 minutes and put it in the gauze? Alright, so now we’re going to proceed with the diagnostic arthroscopy.
CHAPTER 4
So first for the ACL reconstruction, I like it high and lateral right next to the patellar tendon. And I actually do this within the wound itself. You don’t have to make a separate incision. You actually can just go over the bottom. The patella is right here. The top end it right here, so can just basically make an incision. Just go down into the notch like that, and then you put the scope in.
Alright so I’m going to do a small amount, I usually like to create a superomedial portal for the ACL for outflow so you can see a little better. You can see the spot on the video, you can see go in over here. Knife, please. So number 1 blade, just a very small knick-incision going into the cap so we can see right there. Okay, now get the outflow here, and see right there, here’s the outflow. And we’re going to hook this up, kind of helps you clear some of the inflammation in the knee joint.
Ok so, here’s the diagnostics of the arthroscopy. So first thing you do, you go into the patellofemoral pouch and you can see there’s a little bit of inflammation here. That's probably due to the injury that he has over here. And next thing you do is, you can look up at the patella. You can see here. Actually, can you hold this over here for me? Like right there is perfect. Okay, his patella looks pretty good. I’ll take a picture here. And you can go to the lateral gutter, if you can. Sometimes it’s too tight, you can’t, and I think for this kit it might be a little tight so we’ll look at it when we’re getting into the medial compartment and when we put it on figure 4.
So here’s coming down to the medial compartment. Here’s the plateau, you can see it here. We’re going to drop into the medial compartment here. Okay, so you can see here’s the condyle. It’s pretty good. Do not see any lesions here. And the tibia plateau. You can see there’s a little bit of a fraying here to a degree that’s a 1 or 2 on the grading scale, outerbridge. And here’s the medial side here, and let a little bit of a flow go through.
Okay, so now you can see the notch. Here’s what’s left of the ACL. You can see it’s completely torn over here, and then we’re going to start here. We’re going to do a anteromedial portal. Can I have a spinal needle, please? Okay, it’s going to be somewhere in this region here. You want to be able to go and get to a notch. You can see over here, and you can see here. And you want to be able to get to your drilling position, which is going to be on the wall over here.
If you’re going to do a meniscectomy, you want to be just above the meniscus and you're able to go back into position. So I think this portal would be good for both meniscectomy and anteromedial drilling. And I’ll probably go just a little bit more medial to that. Knife, please. So first, I’m going to do just the skin incision here, just on the skin. And then what we’re going to do is go ahead and do an arthrotomy. You’re going to see the knife coming in and then I’m just going to make a little cut on top, so you can through the soft tissue here. Good. Okay, this comes out. Probe, please.
So after an arthrotomy, capsulotomy, you can put the probe in. It’s much easier to put in. Put it in the back. You look into the back of the condyle here. Focus. Over here, a little bit of flow in. And then we’re just going to get, can give me a little bit of Valgus stress here? Okay, that’s good. So I’ll put it right here. Yeah, that’s good. Okay, you can see the meniscus here. It’s intact in the back. No tears, nice, and intact there, so I’ll take a picture. And then over here is a little blunting, but there’s no tear in that region. You can see on top, looks pretty good. You can see that’s pretty good. Does not extrude, there’s no tear over there, and you can put this on top. Looks pretty good there. Okay, so then this looks pretty good. Doesn’t look like there is any tear in the back, that’s very stable. Nothing you need do there. Here’s good. So he does have a little fraying damage in the condyle here as you can see. I would call that grade 1 or 2.
So now here into a notch. You can see here’s the remnant of the ACL that’s completely torn, right here. Okay, let me get a - you can see there’s an empty wall sign right there - let me get an orthocure(articure) 31:35, please. You can see here’s the tear of the ACL here, some of the remnants over here, and you can see there is nothing on the wall here, so we call it empty wall sign(correct) 31:48. Over here, the entire ACL is avulsed and torn off the wall. You can see over here, there is no ACL in the footprint and it’s avulsed off. So now I’m just going to clean off the footprint here. You can see nothing. ACL originally should be inserted right around this region, but there is nothing there. You want to get to the back. Okay, good. So that’s a wall here.
So now what we’re going to do is we’re going to go around to the lateral compartment and take a look at the lateral meniscus. Okay, probe. Okay, I put the probe here. I’m going to go over here. Can you give me a figure 4, please? Alright, nicely, feel my-Give me a nice and easy figure 4. Okay, and then the figure 4 positioning. Good, perfect. Okay, you can see here’s the lateral meniscus. It’s pretty good. There’s a little bit of fraying here. A little tiny fraying here, but it’s very stable, so I wouldn’t do anything there, just a little bit of radial frays. Looks pretty good and if you look on top, there’s no tear on the back. Very stable. I see just a tiny bit of radial tear. We could actual trim that to make that a little bit round here.
So I would call this actually in the segment D on the lateral meniscus and between zones 2 and 3, it’s a little radial tear. Bend it more. Yeah, there you go. Good, thanks. Just a tiny little bit here. So I’m just going to do very minimal trimming here, right there. Okay, good. That’s it right there. I think that’s pretty stable there, wouldn’t do more of it than that. Alright, so condyle looks good on the lateral side. Now we’re going to do the notchplasty and get ready for the ACL positioning. So can we drop the foot of the bed up please, get ready for the ACL. Foot of bed down, trendelenburg, and then foot of bed down, if you don’t mind.
Okay, so this is the ACL right here, here’s some of the remnant. Anteromedial bundles around this region, posterolateral back here. And you can see it’s completely avulsed off the walls. This is what we call empty wall sign. I cleaned off some of the scar tissue in there, and the ACL is completely off. Here is the PCL, right here. It’s made of the anterolateral bundle and posteromedial bundle. Anterolateral is more up high, and posteromedial is more below there. You can see that it’s intact, okay. Could I get an orthocure? So here, I’m cleaning up the footprint in here. Alright, be very careful for the antero-meniscus ligament, so you don’t touch that. So it’s off the footprint right there. I like to open this region up here. It’s where I’m going to put my tunnel. You can see here, meniscus in the front and a little bit of the ACL here. So I-I like it right here, just on the medial aspect of the spine. Right there, okay. You have a shaver?
I’m taking down some of this remnant of the tissue. So I do a very minimal notchplasty here. I actually just smooth out the wall here. Mind if can I get the bone cutter? Thank you buddy, appreciate it. Okay, so this is a little more aggressive. Nice. So I’m just going to smooth the wall a little bit here. The reason I do that is because when you do a-a guide off the back wall over the top guide, you need this wall to be smooth for it to actually sit on it flush. Otherwise, it doesn’t sit very well, so you have to smooth this area out a little bit. Okay, good. Alright so, spinal needle please.
You can see, here’s the-here’s the view, when you do a lateral pull to the patellar tendon. You can see, you typically don’t see the walls well, so what I’ve been doing is I’m actually starting to modifying this view and doing a trans-patellar tendon, and actually, right through the trans-harvest site, just above the notch. So this is the spinal needle and this is where I’m going to put my portal for my scope, so I can actually see much better on the wall and where I make a positioning on the wall, so you can have more accurate positioning here. So here’s it going in. Okay, so right through the middle part of the tendon. You can see over here, right through that region where we did the harvest.
And now we pull back, and you can see the difference. Now you can see, here’s the wall and you can see a huge difference in the visualization and where you want to put the tunnel. And now you can see the entire footprint in the wall right there. And if you want to go back, here is the posterolateral and posteromedial aspect of the knee joint. So you can see, now you can see the notch very well. This is the 12 o’clock position. We’re in the right knee. Here is the 9 o’clock position. And typically in the old days, a lot of the ACLs were put into the noon position over here, or the 11:30 position, becomes a more vertical tunnel. It give you good A-B stability, but in terms of rotational stability, it doesn’t do as well.
So what I do is I do a 10:30 on a right knee and 1:30 on a left knee. So if you look at here, this is a 12 o’clock, 9 o’clock, and a 10:30 position is somewhere right around this region. And you want to be about 2 millimeters of back wall, so if I’m using a 10 millimeter tunnel, I divide that by-by 2, it becomes 5 millimeters and I use over the top guide as 7, so that gives me a 2 millimeter back wall in the back. And here’s the top again, this is at 12 o’clock, here is the 9 o’clock, and my positioning here is going to be at the 10:30 position, which is going to be somewhere around this region. And that restores the posterolateral bundle better, and which it gives more rotational stability for the patient. So give me an arthroscopic alt, please.
I use the arthroscopic alt to kind of show me the position that I want to be when I drill my tunnel. You can see here, so here is the back over the back right here. Looking there...Okay. And then I’m going to mark my spot, which is going to be somewhere in this region, and I like to look a little bit down like that, so I can get the nice view. You can see that’s about the 10:30 position for me right here on the wall, and now I got plenty of space in the back. That’s probably 7 millimeters in front. Okay, go ahead. Mallet that in. Okay, good. Stop. Okay, so that marks the position where I want to be. Right here, you can see that’s a perfectly marked position right there. And that’s going to restore the obliquity very nice, that’s about 10:30 right here. Okay? So over the top, 7 millimeter reamer. Okay, so this is a green 7 millimeter right, over the top guide. I put this in through the anteromedial portal. Okay, so go ahead, so can you just flex the knee up just a little bit.
So the advantage of this system, you don’t have to hyperflex the knee. You just have to flex it just a little bit about nine, a little bit more, just about 90 a little bit over. And you can see now when you flex the knee, you can see where my marking spot is. And when you have the knee in 70 degrees or 80 degrees flexion, when you hyperflex it a little bit the spot moves. So that’s why I mark it with arthroscopic, I’ll identify where exactly I want that spot when I’m looking at the knee straight on and the notch. And you can see here, this wire here on top shows you where on the femur it’s going to come out. And then you can see there’s my spot right there, looks very clear. And then this is over the back right here. Ok I’m going to show you here.
So this thing is going to hook over the back. You see that? That’s over the back wall here. I’m going to hook that over the back, and I’ll move this to show myself here and that’s where I want to be. Okay, so I’m hooked over the back wall. I’m actually perfectly aligned for where I’m gonna be right there and she’s going to drill this pen across. Go. Okay, good. Keep going. Okay, keep going. And then until you come out the other side. Keep going. Go, go, go. Keep going. Keep going. Yep, keep going. Perfect. Okay, good.
So come out, go through. Okay, good. Go through more. Okay good, a little bit more. Okay perfect, right there. Alright, so now you can see the flexible reamer, pen here. We’re going to take this out. It’s exactly where I marked it, 7 millimeters. Okay. The pen is flexible, so it’s easy. You avoid the condyle when you actually go in there with a-with a-reamer. You can see here the positioning is exactly where I marked it on the arthroscopic alt. If you look here, it’s going to be right at the 10:30 position right there. Okay, so let’s do the 10 millimeter diameter reamer. Okay, so go thread this on, and then we should do it by hand to get in, so that you don’t damage the condyle.
So it’s a twisting motion. You twist like this and twist, twist, twist to push in. Okay, and that makes it go in. And when you do that you want to make sure you don’t hit the condyle, which you don’t right there. Okay, can you flex the knee up for a little, buddy, just a little bit. Okay, so back up a little bit. Okay, and then go ahead and right there full speed when you’re just, before you hit the wall. So, go right there. Yep, yeah go ahead. Good, go 5 millimeters. Come back, stop, and then come back out. Okay, a little bit more. Okay, go, go, go. Go 10, and then yep. Good, come back out a little bit. Okay, good, so you can see there’s a good back wall there. Okay, so you got plenty of back wall that’s 2 millimeters. Go ahead go. And then stop at 25, so go. Go more, yep. Stop for a second. Okay, so you’re only at 10, go more. Nice and smooth. Nice and slow. Don’t go past 25, I like the drill that’s about 25. Spin it, a bit more. Yeah, go a little bit more. So that’s 15, okay keep going. Okay, so 20 is here, so keep going to that second line. So go, okay stop. Go one more. Okay, 5 there. Okay, go more so that 25 is flush to bone.
Okay, so now I’ll put this bone cutter in there. Okay, so now what we’re going to do is we’re going to go ahead and this is just going to shave. Okay, this is going basically just irrigate some of the debris out of the tunnel for me. Okay, good. Okay, good. So now you can see this very nice tunnel. You got a nice back wall, it’s about 2 millimeters. You can actually see the tunnel with this portal. You can see strictly up the tunnel, which is very nice especially if you’re going to do a flip-cutter or tight-rope technique. You can drill the pin across here, a foot millimeter pin, you can flip the button and actually see the button flip, and go on the cortex without using C-arm guidance. So this is a very nice portal to view for your intramural drilling, and you can see it’s at the perfect position right here.
So let’s pass a wire for me please. Okay, so now we’re going to pass-we’re going to those two limbs across. And then I’m going to hold the loop right on it. You’ll get a snap. Good job. Nice, very nice. So I’ll hold this loop here. Just right on the tibia here and you can let go of your side. Okay and you’re going to pull. Okay, perfect. So that passes the loop across. And then what I do is I take this loop, I put it over, and then just go snap it right here for me. On top. Okay, so that’s the femoral tunnel, now we’re going to do the tibial tunnel.
CHAPTER 5
So go ahead, this is right here. You can see where my positioning, right there. Osteocure, please. You got it? I’m just going to debride this a little bit here. Okay, so here’s the footprint on the ACL right here. I like it just right here on the medial tibial spine. Just a little bit on the spine, so that is recreates obliquity. You don’t want to be too posterior, if you’re too posterior, you’re going to have a vertical tunnel. You want to be a little bit anterior and a little bit medial, so you get that obliquity of the tunnel there. I use a guide set at 55. So, the patient’s graft is 45. I go with 10 degrees higher than that, so that sets it at 55 for me for the tunnel. Alright, so, and I use a guide that has to the point, so there is one to the elbow, which is marked with a black line. There’s one to the point. I like to the point, it’s more accurate for me. Can I have the table up, please? Oh, watch out for that side over there.
I’m going to go right, kind of on the medial tibial spine right here. Try to recreate this obliquity to the tunnel right there and you want to be just at the footprint. Just going to be right about in this region there. Okay, go on the front and back. Can you feel the back and make sure you’re on the middle bone and not sliding off posteriorly. And you can see, this is the advantage of doing two independent incisions. You can harvest the graft and then you don’t have to fuss around with this area here. You can just do an independent small incision there to actually create your tibial tunnel. Okay, you can go a little bit more, that’s probably a centimeter, a centimeter would be good. Okay, perfect.
So now go ahead and take a Bovie, and just Bovie that and open that down to the bone. Good, so we Bovie that all the way down to the bone and do you have an elevator for me? Okay, that’s good. Okay, on the bone. Good and just take a small elevator and what you do is elevate this off a little bit over here. And go ahead and you elevate that side, so we’re down to the bone. So this helps you so you don’t go through a lot of periosteum and soft tissue in that region, and it hinges you up when you drill the tunnel. Okay, good. So now I’m going to put the guide back and see the tibia here. Put this here. Okay, so this is going to be right footprint. Here’s the tibial spine and this footprint, so I’m going to put it right over here, which is going to be just a little bit on the spine. And it’s going to try to create obliquity and you can see my hand is like tilting towards the- femur tunnel there, okay. Okay and when you hit the tip stop, and then I’m going to take the tip out because you don’t want to ricochet off the tip.
A little bit more. Okay, good. Stop, perfect. So I’m going to take this out, you can take that out. I’m going to take this out and you can see there’s plenty of tunnel, so grab this. And we’re just going to mallet up. And you can see this is pretty nice. It’s already coming towards the obliquity of the- the tibia is off, a little bit off the tibial spine here in front and it’s coming over there, so that’s a good tunnel position right there. Okay, so now we got a needle driver I’m going to grab this pin, and then she’s going to go and do a 10.5 tunnel. Okay, good. Let me make sure you don’t get the skin and you don’t want to- You just want to be, you know, like flush. And it’s actually easier if you do this. Turn your hand there. Gangster style, yeah.
Okay, so you’re flush and you’re not twisting the drill or anything like that. Okay, make sure you’re feeling that. It’s probably like this. It’s like that. So that’s the direction you want to drill. Okay, so, full speed both hands. Okay, okay. Go, both hands. Good, keep going. Keep going, keep going. Good, good. You’re doing great. Nice and easy. Don’t plunge. Okay, good. You’re coming through, good. Nice and easy. Very nice. Oh, very nice. And then spin it there for a second. Okay, good and then come out by hand. Good, okay. Okay, so let me get a shaver. Osteocure first, and then a shaver. So I’ll take the Osteocure and I’ll go right here in the tunnel. I’ll find my position in the tunnel. There it is, right there. And we’re going to clean out just the tunnel here. We’re here, here’s the tunnel there. We’re going to clean that out. Okay, then go on top and do the same thing here. Want to put a curette maybe I don’t know.
Okay, good. You can see here’s the tibial tunnel right here. Okay, let me have a bone cutter. Okay, put a curette there. Very nice. We’re going to put a bone cutter here. Okay, so I like to just basically debride this part. Usually there is a little ridge of bone, so I just to debride that a little bit there so the graft will go passed it a little better. Okay, good. Okay so now you can see, here’s the tibial tunnel right there. It’s very good positioning. Femoral tunnel there. You can see the top, you can see the back wall. Okay, so let’s grab, let me get a shaver. I’m going to get rid of this, some of this stuff here. Okay, good. So I usually like to take an osteocure and just go right at the tunnel. And then I just clean out the tunnel here. This opens the tunnels up for you without impinging on the soft tissue, so it just goes on top. This works really well, so you get rid of all the soft tissue around the tunnel just at the opening. Okay.
CHAPTER 6
So now you take a loop-grasper, which is a ring-grasper. You go through the tunnel here. And you grab these sutures. Okay, go ahead untangle that. Unhook that and hold your side. Okay, hold that side. Very good, okay. So now you got the tunnel here. Okay, let me see the graft. So I’m going to double-check the graft because every time you put it into solution it may actually swell up. So I double-check myself to make sure it doesn’t get any bigger before I pass it because that’s important. You don’t want it to get stuck up into that region. So, here’s a 10. Can you hold this for a second? And here’s a 10 right here and it’s going through a 10 very easily. And then this is the 10 here, which is going through very nice and we drilled a 10.5, so I’m not worried about it. So that’s going to be good. And this is the side with an orthocord, which is going to be my side for the femur.
So hold this graft for a second.Yeah, that’s fine to let go. Yeah, that’s fine. That’s alright. We’re going to float, we’re going to swim today. It’s not a big deal, not a big deal. Okay, so this is going to go over here. We’re going to put the loop around. Okay, and then I’m going to hold this part of the graft, you can see. Okay, so let go. Okay, so go ahead. Pull that out. Yeah, you let go. And then pull your side out. Okay, ready? Okay, you can see here, go. Look at it, yep. Okay, yep go. Pull, pull, pull. Go, go, go, go, go. Keep going, yep. Keep going, good. Keep going, perfect.
Alright, so now we got the graft passed. You want to just show me here. Okay, so I got this and you just got the camera. That’s good, so perfect. So now you can see the graft. So I like the graft facing me because I like the bone plug facing me, and then the screw on top of the bone crust. So it’s facing me right now and then you go through the tunnel. And this should be going pretty easily and because I actually made it smaller. Here’s the graft coming in. Take a picture for me. You can see it. See, you can see this, when I did this little ridge right there, that little ridge makes it really nicely, easy to turn it. And now you pull it through and it’s going to go right across right there. Okay, you see it’s going to go right there, perfectly go into it just like that. Okay, so now there’s the ACL. So it’s much easier to do that when you make the tunnel just a little bit smaller. So now we got the ACL in there.
So now I’m going to do an interference screw, so we’re going to get this up here. Perfect. Okay, so now let’s get the notcher. This is going to be a 7 by 20. Yeah, 7 by it’s 20. Metal, metal. 7 by it’s 20, I think. Okay, so can you flex the knee for me ma’am, if you don’t mind. Hold on one second. Let me, okay, so just flex it a little bit more. That’s good. So you can see, that’s the graft. I want to be in front of it. I want the screw in the position basically in front of the graft and pushing it down, se we recreate more of the obliquity. So that position is good. There’s the screw, so I put it right there. And you can see this nice position right there. Go ahead. So she’s going to notch it. Keep going, keep going. Okay, good. Stop. Okay good. And then guide wire.
Alright, so here is the guide right here coming in. Make sure you can see the bone graft. So I want to be in front of it. Just going to be right, I think right there it probably pretty good. See if you can get it up there. Is it going in or no? Okay, so see if you can tap it in. So put a little bit, just very small increments because I think if you do too big it may bend. Yep, perfect. Okay, so just tap it in. It should go in easy. Okay, good. A little bit more, increment. Okay, good. Let’s try that. See if it finds the hole right there. Okay, let’s see if it feels like good.
Alright, so we’re going to spin it in right here. Over here, you can pull that here, please? Okay, so here’s the screw going in. Right here, and it’s perfect. Here’s the screw going in, the interference screw, right. Superior to the graft and you can see there is a very good bite here. It’s nice and tight. Okay, so that’s very good. So take a feel here. Elena, take a feel, take a feel. So you can’t really turn much more than that, right. So, mallet please. Get the mallet and tap this out for me.
Okay, good. Tap, tap, tap, tap. Good, alright. Perfect, so now get the wire for the needle driver and take that out. Mallet. So you can see over here that here’s the screw. It’s in front of the graft right here on the wall. And you can see that if I’m in this portal, this position here, which is right next to the patellar tendon on the lateral side, you don’t see the wall as-as well. But so that’s why when we do the portal up here in the notch, you can see here’s the notch right here, the view, original view that we used. And then you can see the difference, so here’s the wall over here. And you can see literally you’re looking at straight onto the wall of the lateral femoral condyle. You can see the screw right there. The graft is behind it. It’s superior, anterior to the graft. It pushes it even down to recreate the posterolateral bundle. And here’s the ACL right here. Okay, and then I’m just going to get. Okay, just take a look. So you can see here’s the ACL going up, and there’s no impingement right here. Superiorly, it’s not impinging a notch. You always want to check for that. Okay.
Okay, so I’m going to, we’ll tension the tibia side and then I’m going to go back and we’re going to clean up a little bit of the ACL, so you get a better picture of it. Alright, so the tensioning of the ACL. You can see this graft’s very nicely taut. I like to cycle the graft about 20 times. I think that reduces some of the creak in it. So, one, two. Okay, so that’s about 20. And then you come up here, and let me have the bump. Okay, so put the bump underneath the thigh. We’re going to do about 20 degrees of flexion. Okay, like right there. Okay, good. And then could I get a army-navy, or like something-Senn’s over here, and then suction. Alright, you can see the bone plug is very nicely and perfectly matched into the tunnel right here. It’s flush.
So in the cases that if you have a tendon-tunnel mismatch. What you can do is, a couple things you can do. If you have mismatch 5 or 6 millimeters you can actually twist the graft. So you can actually take the two and twist it up to 5 or 6 times, so that you can shorten the graft. So that’s one way to do it. If the graft is mismatched by 4, 5 or 8 or 10 millimeters. What you can do is, you can take actually take a Richards staple. You put a screw in there and you take the Richards staple and staple it down. You can take an osteotome, a curved osteotome, make a trough put a down tension in it and take a staple. If the bone plugs are completely out of the tunnel, couple things you could do, you can cut the bone plug off and you can put a soft tissue interference screw and do a back-up fixation after that. Or you can actually use the bone plug, make a trough distally in the tibia, and then you can put two Richards staples down, with tension and graft. All those techniques can help when you have a mismatch. In this case, the one plug is actually perfectly flush here on the tibial tunnel.
So now what we do is, I’m going to have pulling-tensioning here. I’m going to put, I’m go to ahead and put, where’s that pin for that? Hey, can you give me that pin in that-2 Okay, so I got the pin here. So this pin is going to go just underneath the bone plug right here. I need a little suction, and you can see there’s a little, nice hole for where the graft wants to go. So let me see the screw. Do you have the screw? Ah, right there. Okay, so here’s the screw. It’s an 8 by 25. So I use the 8 by 25 on this side, and the reasoning is that you’re not worried about blowing out the posterior wall of the femur. So you can go a little bit bigger. If you’re using a 10 millimeter tunnel, femoral side, I usually go down to a 7 millimeter screw because I’m worried about blowing out the back wall. So that usually works out very well for me. Okay, so I’m putting tension here. Can you come over here for a second? Just give me a little posterior drawer, so push back on the tibia like this. Just put your hand here, just a little right there. Okay, that’s good.
So she’s giving me a little posterior drawer. And then I actually check in extension, and the reason I check in extension is that if the graft actually pulls back in extension that means that it’s impinging extension and I actually tension in extension so you don’t over capture the knee. So right now the graft is very isometric, so it doesn’t move at all. So I know that 20 degrees with posterior drawer that’s going to be the best place to tension this graft, at this point. So she’s pushing posterior drawer here, so a little bit back. She’s holding on. This is a 8 millimeter screw here, so I’m going to go ahead and put that in. Okay, good. This comes out. Okay, let me get a needle driver and a mallet. So you can see here the screw right over the bone part, it sticks out. Very nice. So I leave these things here just for now. So you want to do a Lachman at 25, 30, 20 degrees or so. You can feel, and you can feel you recreated the knee as stable as it can be.
So now, what I want to do is after the ACL reconstruction, I want to check and make sure I’m not impinging over here. Especially, if the screw is protruding, tibial tunnel, you can see there’s no screw. It’s in there. The graft itself is nice and taut, you can see here. And then using this portal I’m able to visualize the femoral wall. And you can see the screw in front of the graft right there. Next thing you want to do, you want to make sure it doesn’t impinge the extension. So you take the knee and you follow the graft, and you want to see that it doesn’t hit the notch. And you can see right there it’s nice-nice and flush. It does not impinge on the notch right there and the leg is in full extension right now. Okay, and then it comes down, graft is, it should reduce it right here.
And then this is low on the wall, it’s called 10:30, but when you put the screw on top, in front of the graft, it actually pushes down even lower than 10:30 to recreate that posterolateral bundle. So it restores the rotational stability of the knee much better than a vertical tunnel or a tunnel that’s at a 12 o’clock or 11:30 position. This is at a 10:30 position right here. Okay, good.
CHAPTER 7
So I like to put a couple of interrupted stitches in a tendon. And what I do is, it’s going to be just on the edge. You don’t want to over tension it. Here. Okay, thanks. It’s good. Alright, so now we’re just going to put this interrupted. Cut. Scissors, please. Thanks, you just want to come over here? Okay, same thing. Pickup. So now we’re going to do a little bit of a-grab a pickup. Can I get a pickup? We’re going to put the bone graft in the patella, defect region, if you have some bone, extra bone, you can always put it in this part, so let it heal a little better. So, okay. Okay, more.
Alright, so I try to close the paratenon if you can. So you find this layer on top and close it over the tendon here. You really can’t, it doesn’t go. Just close the paratenon. And I typically just run the stitch here if I can. Lift up for a second. So here’s the paratenon there, here’s the paratenon here. Okay, and you can see it closes nicely over the bone graft, patella there. Thank you. So I typically just run this paratenon if you can, just over the tendon. It’s actually nice, really nice on this guy. Okay, so this actually closed up really nice, this guy.
So you can see now the paratenon is nicely closed over the patellar tendon right here on top and bottom. And then what I’m going to do is I’m going to get, let’s do 3-0 vicryl. So I like the 3-0 vicryl stitches because they have a shorter life and half-life dissolving. So I do 3-0 vicryl interrupted and I run 3-0 vicryl. Okay, so now we’re going to just check the Lachman exam after we did this case. So you can get a full extension, and then 30 degrees here and you can see nothing, no translation at all. I’d call this a 1A Lachman. Good end point, it’s very solid. Nothing at all. And I typically don’t pivot them on the table after the procedure. Just, I think that’s too much stress onto the graft.