
Bilateral Modified Radical Neck Dissection for Metastatic Papillary Thyroid Carcinoma
Main Text
Table of Contents
Radical neck dissection was once the standard of care for the surgical management of patients with thyroid cancer and cervical lymph node metastases. However, due to the significant morbidity of this procedure, the development of cervical lymphadenectomy procedures that could provide oncologic cure while minimizing morbidity was undertaken by many surgeons. Such an investigation has led to the development of the modified radical neck dissection (MRND). Still, many institutions are not familiar with performing a comprehensive MRND in the setting of thyroid cancer metastatic to the lateral lymph node compartments. We present such an operation under general anesthesia.
Cervical lymphadenopathy; cervical lymph node metastases; modified radical neck dissection.
Thyroid cancer is the most common endocrine malignancy in the U.S. The rate of new cases has been steadily rising over the past several decades, with the vast majority being papillary thyroid carcinomas (PTC).1,2 The most common route of spread of PTC is to cervical lymph nodes; up to 40–90% of patients with PTC have evidence of cervical lymphadenopathy at the time of diagnosis.3
The patient is a 61-year-old male who presents with bilateral persistent metastatic PTC to the bilateral lateral neck lymph node compartments. In 2014, he had undergone thyroid cancer screening after his brother and sister were found to have papillary thyroid cancer. At an outside institution, he had a total thyroidectomy in March 2014, at which time the right thyroid PTC was noted to have adhered to the right recurrent laryngeal nerve. The final pathology showed bilateral PTC with the largest tumor measuring 3.1 cm on the left side with extrathyroidal extension. 3 of 6 lymph nodes contained PTC. Preoperatively, he had undergone a CT scan of the neck that clearly demonstrated bilateral lateral neck lymphadenopathy consistent with metastatic disease (Figure 1). However, the lateral neck disease was, for unknown reasons, never addressed at the initial operation. He had trouble with his voice after surgery and still had issues with voice fatigue postoperatively. He was treated with radioactive iodine 134mCi in April 2014. He had no evidence of metastatic disease on the post-treatment iodine scan, but thyroglobulin levels were persistently elevated.
His course was unremarkable for the initial years, but then in 2017, an ultrasound showed bilateral level III lymph nodes with calcifications. They were possibly slightly enlarged compared with previous imaging, but thyroglobulin levels were unchanged. In April 2018, he underwent a comprehensive ultrasound with lymph node mapping, demonstrating lymph nodes concerning for metastatic PTC in bilateral lateral neck compartments (i.e. lymph node compartment levels II–V). At this time, the thyroglobulin level was elevated at 48, with a thyroglobulin antibody titer of less than 10. Fine needle aspiration (FNA) biopsies of the right level IV and left level III lymph nodes were performed, and both were positive for PTC, proving that the patient had bilateral recurrent metastatic PTC to the bilateral lateral neck lymph node compartments. In addition, CT scans of the neck and chest with and without IV contrast were also consistent with these findings. At this time, he was referred to Yale Endocrine Surgery for consideration of remedial surgery. There were no other complaints of hoarseness, difficulty swallowing, or breathing.
The biochemical evaluation demonstrated a normal TSH of 1.13, elevated thyroglobulin at 48 (unstimulated; without positive thyroglobulin antibodies), and total serum calcium of 9.4 mg/dl (reference range 8.8-10.2 mg/dl).
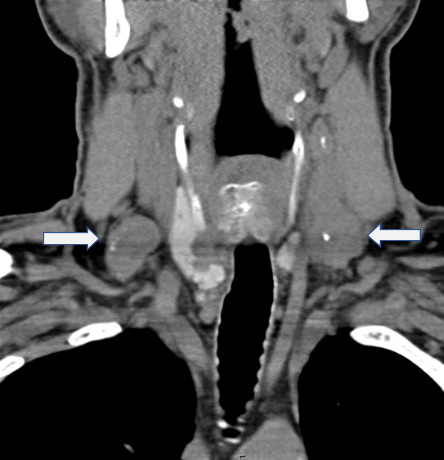
Figure 1. CT scan of the neck from 2014.
Positive lymphadenopathy in the bilateral cervical lymph node compartments (arrows).
Unfortunately, these were not resected at the initial operation performed at an outside institution.
A comprehensive ultrasound with lymph node mapping was performed, demonstrating lymph nodes concerning for metastatic PTC in bilateral lateral neck compartments (i.e. lymph node compartment levels II–V). Fine needle aspiration (FNA) biopsies were performed of the largest right level IV (measuring 2.8 x 1.9 x 1.8 cm, with extension into the level V lymph node compartment) and left level III lymph nodes (measuring 3.7 x 2.1 x 2.9 cm, with extension into the level V lymph node compartment, as well), and both were positive for PTC.
He underwent a CT scan of the neck and chest, which demonstrated abnormal lymph nodes in the neck soft tissues, some demonstrating pathological enlargement, calcifications, and central necrosis, concerning for metastatic disease. Representative examples included a 3-cm left level III lymph node, which narrows the adjacent internal jugular vein, a 2.1-cm right level 3 lymph node, a 9-mm left level II/III lymph node anterior to the carotid space, with possible lymph node abutting the bifurcation of the right subclavian and right internal jugular veins, and a 1.7-cm left level IV/supraclavicular lymph node.
The presence of cervical lymph node metastases in thyroid cancer portends a decreased survival rate as compared to its absence.4 Accordingly, lateral neck lymph node dissection remains a mainstay in the surgical treatment of this disease process.
Surgery is the only primary treatment for metastatic PTC. However, adjuvant radioactive iodine therapy (RAI) is often instituted to treat persistent microscopic disease, as well as ultrasound-guided alcohol ablation in select cases.5 Occasionally, when surgery is not possible, palliative external beam radiation therapy is used.
Radical neck dissection (RND) was first described by George Crile in 1906 and has remained the standard of care for the treatment of cervical metastases in head and neck squamous cell cancers.6 The standard procedure involves the removal of lymph nodes in all compartments of the lateral neck (levels I through V), as well as resection of the spinal accessory nerve (SAN), internal jugular vein (IJV), and sternocleidomastoid muscle (SCM). The procedure is associated with substantial long-term disability, including shoulder dysmotility and cosmetic deformity.7 Because of the significant morbidity of this procedure, efforts have been undertaken to provide alternative surgical approaches that are equally efficacious but less morbid than the standard RND.
Two alternative procedures that have been developed include the modified radical neck dissection (MRND) and selective neck dissection (SND). Modified radical neck dissection involves the removal of all lymph nodes typically removed in the RND, with sparing or preservation of at least one of the following structures: SAN, IJV, SCM. A selective neck dissection refers to a cervical lymphadenectomy in which there is the preservation of one or more of the lymph node groups that are routinely removed in the radical neck dissection. To date, no prospective randomized trials comparing RND to either MRND or SND exist. However, there are several retrospective studies comparing outcomes after RND versus MRND; mean combined recurrence rates were significantly lower in the MRND groups [6.9%, 95% confidence interval, 5.4–8.4%] as compared to the RND groups [13.6%, 95% confidence interval, 12.0–15.2%].8
In the setting of metastatic PTC, cervical lymphadenopathy remains the most common source of disease recurrence or persistence.9 Therefore, adequate cervical lymphadenectomy is a primary determinant of outcomes after surgery. However, significant controversy remains regarding the extent of lateral neck dissection that is necessary to achieve optimal outcomes. A study by Caron et al.10 suggested that there is a much higher incidence of lymph node involvement of levels III and IV, and therefore SND is adequate in most cases of metastatic PTC. One criticism of this study is that only a small number of patients were included. We recently demonstrated in an extensive series of MRND procedures at a single institution that omitting levels II and V potentially leaves behind the disease in 67% and 20% of patients, respectively; therefore, MRND is the optimal procedure to minimize the morbidity associated with reoperative surgery for missed disease.11
Surgeons performing MRND must have a thorough understanding of the anatomy of the neck, as well as embryology of the parathyroid glands. In general, MRND is indicated whenever preservation of the SAN, SCM, or IJV is possible without compromising a complete oncologic resection.
A transverse (Kocher) incision is created and extended laterally along the lateral neck. In this particular patient, the previous scar was excised to ensure the best possible cosmetic outcome. Subplatysmal flaps are elevated superiorly and inferiorly. The greater auricular nerve is identified and then followed to Erb's point (it is located on the posterior border of the sternocleidomastoid muscle, approximately 2–3 cm above the clavicle, where the greater auricular, lesser occipital, transverse cervical, and supraclavicular nerves emerge. It is a critical landmark for identifying the spinal accessory nerve) and is preserved. Approximately 1.5 cm above Erb's point, the SAN is identified. The SAN is then carefully dissected out and preserved as it enters the trapezius muscle. As the SAN exits the anterior triangle and enters the posterior triangle, it crosses over the GAN under the surface of the sternocleidomastoid muscle forming an imaginary cross (“X-pointer”). At the posterior border of the SCM, the SAN is found superior to the GAN and this relationship gets reversed at the anterior border. The cervical rootlets often have a similar course as that of the accessory nerve and can confuse the surgeon. In this context, X-pointer is an additional dependable, constant and easy landmark to differentiate the SAN from the other nerves; it is independent of body proportions.12 Other landmarks for SAN identifications are the followings:
- The SAN in relationship to the IJV is coursing dorsally in 44% and ventrally in 56% cases (Kierner et al.).
- The contribution of the cervical plexus to the SAN is primarily from the C2, C3, and a combination of the two and has communication to the nerve deep to the SCM muscle in the posterior triangle.
- Shiozaki et al. reported three types of innervations to the SCM muscle classified as type A—non-penetrating type, type B—partially penetrating type, and type C—completely penetrating type.
- The mean distance from the midpoint of the clavicle to the point of entry of the SAN into the trapezius muscle is about 59 mm. This is an important landmark for tracing the SAN from the lower neck and dissecting superiorly. The SAN innervated all parts of the trapezius muscle, and hence, the isolation and preservation of the nerve became important.13
The level V lymph node compartment is then mobilized from lateral to medial. The entire cervical fat pad encompassing the level V lymph nodes is dissected free. The external jugular vein is divided superiorly and inferiorly. The fascia is then unwrapped from the SCM. The omohyoid muscle is dissected out and preserved; if necessary for better exposure, it can be sacrificed. The IJV, common carotid artery, and vagus nerve are dissected free and preserved throughout. The specimen is then mobilized from lateral to medial, encompassing all the fibro-fatty lymph node-bearing tissue from levels V, IV, III, and II. Dissection is carried superiorly to the digastric muscle. The glossopharyngeal nerve is identified and preserved. Dissection is carried inferiorly to below the clavicle. In the case of a left-sided lateral dissection, the thoracic duct is identified and preserved; it can also be ligated if necessary. Although there is no dominant lymphatic duct on the right side, care should still be taken during the supraclavicular dissection to avoid a lymphatic/chyle leak. The phrenic nerve is identified medially. It lies lateral to the vagus nerve, and the brachial plexus is identified laterally to the phrenic nerve; both are preserved. Phrenic nerve is an important landmark as it innervates the diaphragm, following the prevertebral fascia during dissection would be helpful for preventing the injury to phrenic nerve. Small branches of the transverse cervical nerves are divided as necessary. The entire specimen is then removed and sent to pathology for the permanent section.
In this particular patient, the cancer significantly adhered to the omohyoid muscle as well as the internal jugular vein in the left level IV lymph node compartment. Despite the well known margins of level IV (anterior margin is lateral border of the sternohyoid muscle, posterior border is the posterior border of SCM, superior border is omohyoid muscle and inferior border is clavicle) the operating surgeon thus resected the internal jugular vein and omohyoid muscle en bloc to achieve negative margins. A surgical drain (#10 Jackson-Pratt) was placed on each side of the neck.
The surgical pathology revealed that the scar revision only contained benign skin with scar. In total, 10 of 34 and 5 of 26 lymph nodes were positive in the left and right MRND specimens, respectively. All lateral neck lymph node compartments (levels II–V) contained at least 1 positive lymph node except for the left level II lymph node compartment. The largest positive lymph node on the left side measured 3.9 cm, and on the right side 3.8 cm. There was evidence of extranodal extension of the PTC in the bilateral lateral neck. At approximately 10 days postoperatively, his bilateral cranial nerves (CN) were all grossly intact (CN II–XII) and his vocal cord function as assessed by flexible laryngoscopy was completely normal. Additionally, his serum calcium was normal at 9.4 mg/dl [reference range 8.8–10.2 mg/dl].
No special equipment was used.
Nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review (CSR) 1975-2016. Bethesda, MD: National Cancer Institute. Available at: http://seer.cancer.gov/csr/1975_2016/.
- Cooper DS, Doherty GM, Haugen BR, et al.; American Thyroid Association Guidelines Taskforce. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006;16(2): 109-142. doi:10.1089/thy.2006.16.109.
- Carling T, Udelsman R. Thyroid cancer. Annu Rev Med. 2014;65:125-137. doi:10.1146/annurev-med-061512-105739.
- Jin S, Bao W, Yang YT, Bai T, Bai Y. Establishing a prediction model for lateral neck lymph node metastasis in patients with papillary thyroid carcinoma. Sci Rep. 2018;8(1):17355. doi:10.1038/s41598-018-35551-9.
- Suh CH, Baek JH, Choi YJ, Lee JH. Efficacy and safety of radiofrequency and ethanol ablation for treating locally recurrent thyroid cancer: a systematic review and meta-analysis. Thyroid. 2016;26(3):420-428. doi:10.1089/thy.2015.0545.
- Crile G. Excision of cancer of the head and neck. With special reference to the plan of dissection based on one hundred and thirty-two operations. JAMA. 1906;XLVII(22):1780-1786. doi:10.1001/jama.1906.25210220006001a.
- Ewing MR, Martin H. Disability following “radical neck dissection”: an assessment based on the postoperative evaluation of 100 patients. Cancer. 1952;5(5):873-883. doi:10.1002/1097-0142(195209)5:5<873::AID-CNCR2820050504>3.0.CO;2-4.
- Buckley JG, Feber T. Surgical treatment of cervical node metastases from squamous carcinoma of the upper aerodigestive tract: evaluation of the evidence for modifications of neck dissection. Head Neck. 2001;23(10):907-915. doi:10.1002/hed.1131.
- Braverman LE, Cooper DS, eds. Werner & Ingbar’s The Thyroid: A Fundamental and Clinical Text. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2013.
- Caron NR, Tan YY, Ogilvie JB, et al. Selective modified radical neck dissection for papillary thyroid cancer—is level I, II and V dissection always necessary? World J Surg. 2006;30(5):833-840. doi:10.1007/s00268-005-0358-5.
- Javid M, Graham E, Malinowski J, et al. Dissection of levels II through V is required for optimal outcomes in patients with lateral neck lymph node metastasis from papillary thyroid carcinoma. J Am Coll Surg. 2016;222(6):1066-1073. doi:10.1016/j.jamcollsurg.2016.02.006.
- Rao V, Subash A, Sinha P, Chatterjee S, Nayar RC. The X-pointer: a forgotten anatomical relationship of spinal accessory nerve and great auricular nerve. Surg Oncol. 2021;37:101522. doi:10.1016/j.suronc.2021.101522.
-
Anehosur V, Kulkarni K, Kumar N. Variations in the anatomy of spinal accessory nerve and its landmarks for identification in neck dissection: a clinical study. J Maxillofac Oral Surg. 2021 Sep;20(3):426-431. doi:10.1007/s12663-021-01542-z.
Cite this article
Courtney Gibson, MD, MS, FACS. Bilateral modified radical neck dissection for metastatic papillary thyroid carcinoma. J Med Insight. 2024;2024(238). https://doi.org/10.24296/jomi/238Procedure Outline
Table of Contents
- Patient positioning.
- Surgical approach and marking.
- Create extended Kocher incision.
- Develop subplatysmal flaps.
- Identify GAN and follow to Erb’s point.
- Identify SAN and follow to insertion to trapezius muscle.
- Mobilize level V compartment from lateral to medial.
- Divide EJV.
- Unwrap fascia around the SCM.
- Circumferentially dissect and preserve carotid sheath contents.
- Further mobilize lymph node specimen from lateral to medial, including levels V, IV, III, and II.
- Identify and preserve (or ligate) thoracic duct (left side) or other minor lymphatic ducts (right).
- Identify and preserve phrenic and brachial plexus nerves.
- Divide transverse cervical nerve branches as necessary for complete mobilization of lymph node specimen.
- Place a drain deep to the SCM for decompression of residual lymphatic fluid.
- Close strap muscles.
- Close platysma muscles.
- Close dermis with 5-0 Prolene.
- Apply Dermabond and Steri-Strips.
- Remove drain once output is less than 30–50 cc and serosanguinous (usually postoperative day 2).
Transcription
CHAPTER 1
So, this is a 61-year-old male, who, back in 2014, at an outside institution, had a total thyroidectomy and central neck dissection, for what proved to be a bilateral papillary thyroid cancer with extrathyroidal extension. He then underwent radioactive iodine and then, via surveillance, he had the follow-up ultrasound. And this is a schematic from the ultrasound showing obvious bulky disease in the right level IV lymph node compartment, as well as the left level II, III, and IV lymph node compartment. Fine needle aspirate of both the right level IV lymph node as well at the left level III lymph node was consistent with papillary thyroid cancer, proving that the patient has recurrent metastatic papillary thyroid cancer to bilateral lateral, uh, neck, uh, compartments. Uh, we don't routinely to do this but he was, um, uh, referred with a CT scan. And this is his CT scan, that gives a few clues. Uh, so this is the right side, this is the left side, this is the jugular vein and carotid artery uh, on the left side. And on the left side you can see there's obvious bulky disease deep to the sternocleidomastoid muscle, and there's almost a disappearance of the internal jugular vein. And then you have contrast coming back, uh, below, below the vein.
CHAPTER 2
The positioning is essentially the same as we do for total thyroidectomies, meaning that the patient is in a beach chair, semi-Fowler position. Uh, we always make sure we prep and drape very widely, to make sure we have access to the high level II lymph nodes as well. So, this is the previous incision that the patient had. It hasn't healed perfectly, so we're going to excise that incision to make sure we have a nice cosmetic outcome. In terms of the landmarks, this is the thyroid cartilage, this is the sternal notch, with the clavicles on each side. So, I'm going to use the old incision and we're going to excise that, and then we're going to bring the incision up on each side, to about 4 cm below the ear lobe. So, here is the external jugular vein on that side, and on this side. So, to make sure we get this symmetrical... Make it a little bit rounder. Now we just mark this out so we can perfectly line the skin up at the end of the operation. All right, so, maybe start from over here. Okay, so, so, we're starting. And then, you just can excise that.
CHAPTER 3
We're starting. So, first specimen is going to be called scar revision. Okay. Continue here. Can I have an Adson, please? But you're making sure we can use the nerve stimulator, right? Yeah. All right, so this is the scar revision. Okay. Okay. Scar revision specimen. Okay, don't be shy, just clean up all this. Let's increase the Bovie to 20 right now. All right, so come through, now. All right, so next we're going to create the subplatysmal flaps, here. But first we want to identify the greater auricular nerve. That's going to be up here. That's the vein, there. So, just open above and below. There's a little bit of scar tissue here in the midline from the previous. So, tilt the table towards me, double skins. So first, we're going to dissect out here the external jugular vein which we're eventually going to sacrifice, but that, that will take us to the greater auricular nerve. Just tilt the table a little bit more towards me. That's good. So, this is the greater auricular nerve right here. So, this is a sensory nerve to the earlobe and, that will bring us back to Erb's point, where we'll find the accessory nerve, about a centimeter and a half superior to the insertion of this nerve. You can just fix that lower light for us. Now we're creating the subplatysmal flaps, here. Really crank that up. All the way down here. As long as I stay right underneath the platysma here it's very safe, and I can go pretty quickly with the Bovie. I think you can get rid of that and then just follow the vein down here. Scissors, and can I have Metz, please. Yep. Okay, so pick that. Pick the whole thing up. Mixter, I'll take a 2. So, just follow that down. Let's just move him down here. Okay.
CHAPTER 4
Yeah, it's not pretty, but I guess we'll be able to do it. So, I'll take a fine tonsil, now. So now, the next order of business is going to be to find the accessory nerves. So, this is the great auricular nerve heading in right at Erb's point. So, about 1.5 cm above this point, Erb's point, we're going to identify deep here the accessory nerve. Just score this a little bit. Bovie. Get the nerve stim here. All right, so we use the nerve stimulator for the motor nerves here, to identify the accessory. All right, so it's right there, deep. We had it there for a sec. Right, I see it now. Okay. Okay. All right, don't get the nerve there. Okay. Pickups. All right, LigaSure to me. So, now we're sacrificing the external jugular vein, here. No, no, just - stay closer to... All right, so tie this. All right, I'll have a Mixter to me. 2-0 tie. Okay, so, next order of business... Take a fine tonsil. We're going to open up the anterior border, here, of the sternocleidomastoid muscle, and mobilize the fascia around the - around the SCM. Stay closer to me, you want to get all that tissue. Just going to put you in a little deeper, there. Just take that for a second, Rob. Okay. Yeah, so, this is all cancer right here. Yep. So, we're going to stay high up in the, the sternocleido. If we have to take a little bit of the posterior aspect of the sternocleido just to get negative margins, we certainly can do that. You want to keep that deep, you don't want to fall out with that. Let's just advance here, a little bit. All right, so, the cancer's a little bit stuck up here on the underside of the sternocleidomastoid muscle. Let's carve through that. We're taking a little bit of muscle with us here, to get sure we get negative margins. And let's carve through that. Yep, just push through it. I'll switch to Mixter now, for a second. Pickups. All right, so let's see if we can advance this even a little bit more. All right let's come from lateral side. So, the cancer's a little bit stuck on the underside of the sternocleidomastoid muscles. We're going to mobilize it from lateral, just to make sure we get all the tumor here. That's tumor there too, okay. Keep that deep in, okay. Okay. I'll take a LigaSure. Let's pick this up. Okay, so you take this. Yep, let's follow the muscle. Okay, so that's all tumor stuck to the... Okay, wow, that's rock hard. So, so, take a feel there. So, rock hard on the underside there. Okay. Stay up in the muscle. Pickups. Let's go - get a clamp - I'll take a fine tonsil to me now. Yep, get all of this out. So this is all cancer up here, so pull a bit harder there. Yep, yep. Okay, that's all cancer there. Okay, that's good. So here, this is all cancer, this is the IJ here. As we could see on the preoperative scan, the IJ might be involved, so, we're going to make a decision whether to sacrifice the internal jugular vein or not, here. Large Penrose. All right, so I'm going to push that tumor down here, so you just follow the muscle here. Just use your finger, push that down. Make sure you stay high up on the muscle. We're down to the clavicle there, so that's good. I'll take that. Take back those. All right, so let's do the omohyoid. So again, this is all tumor, which is unusually hard and adherent here, so... So again, we're going to see if we have to resect the IJ or not. So, now we're dissecting out the omohyoid muscle. I'll take a small Penrose. Follow it up for me. So Mike, you want to hold on to those at all times, right. Mixter. Probably going to sacrifice all that. Take a squirt. Let's just follow that laterally. Put that in there. And Rob, if you take this for a second... So, this is all tumor here, okay. Might have to sacrifice that, too. You know what? Uh, so, because it seems like the omohyoid is involved with the tumor - Yeah, take that. So, usually we preserve the omohyoid, but the cancer laterally here down in level IV is involving the omohyoid muscle, so we're going to resect that en bloc. Take another 2. And then just pass that underneath.
CHAPTER 5
All right, so, to be able to know whether the - Pick, pickups now. Be able to know whether the tumor is invading the IJ or not. So, this is cancer sitting right on top of the IJ. Let's get to it above, here. Take a blunt tonsil to me, now. All right, so this is the space. The question is whether the tumor is involved here, or not. All right, let's just get a vessel loop on it above, first. Yep, yep, so dissect it. So, don't give up on it, continue to hold it. Okay, and then dissect above and below. Mixter. Pickups. This is more tumor right here, so... Yep, this is - I'll take that from you. I'll take a blue vessel loop. All right, just follow it up a little bit more. That's a branch, there, so do this side. Stay a little bit closer to the vein. Okay. I'll take an Allis to me. So, make, you know, 10 buckets, call them left modified radical neck dissections level II, III, IV, and V, and then the same on the right. Here's the digastric muscle right here. Means the hypoglossal nerve is going to be just deep to it, right... Okay. Want to get your nerve stim in? Okay. That's the hypoglossal nerve, right? So, just... I'll take a - yep. Okay, you take that, now. That's the nerve, right, going right underneath that vein, so, let's just tie that. So you hold there. Mixter. Scissors. And just pull that aside. 2-0. Mixter. Just carve that right on the knot. Just use cutting. Okay, that's fine, that's fine. Pickups. All right, flip it that way. We're going to ligate - just bust that. This will release the hypoglossal nerve. Just going to put it right there. Pickups, fine tonsil. Hypoglossal nerve. So, right there, okay. Is that another branch? Looks like it, right? Okay, you take that. Pickups. We'll just see if we can see the vagus now. That's the carotid, so just carve that - yep. Just carve onto the carotid. Just touch that directly. I'll take a squirt. Bovie too much. Scissors and then a 3-0. All right, so a lot of tumor. So, this is all tumor as well, so - just follow the carotid down there. Bovie to me. Okay. DeBakey. We can just let that hang first and let's go find the vagus, and then pull that laterally. Pickups to me. It's going to be down here. Buzz this one please. It's from underneath here, just hold tight here. It's this thing here. We're going to have to ligate that anyway. Let's just... Okay, so if you hold tension on that. Yellow vessel loop, please. I'll take a squirt. We'll just hold some tension on that. All right, so here, we have the hypoglossal nerve crossing - hold it towards you - the carotid bifurcation is right here. The vagus nerve and then the IJ. But this is all cancer here, so, what I'm thinking, we're going to ligate the vein up here, here, and then below. And then we're going to resect that all, the, the IJ, uh, en bloc, so... For this one, now, you can tie that. I'll take a LigaSure to me. All right, so that's good. So, that's as far north we need to go, So, let's pick up - ligate this here. And this, this is all, yeah, that's just muscle. And this is, that's the omo - Yeah, insertion of the omohyoid. So, you can hold that towards you. Okay, so now... Let's find the IJ deep here, now. Scissors Okay. Pickups. Just use some Metz there. Scissors. All right so - all right, LigaSure to me. All is quite stuck here, you know. You want me to try to come through here? Kind of like, lateral, along this border? Or do you want to take it out all together. Yeah, I'm thinking we'll probably resect it all en bloc, there. Because this is the IJ below. Do you want me to get around it down there? I think what we'll do is we'll start mobilizing from lateral to medial and then hopefully we'll be able to get a little bit better exposure down there. And I'll switch to the big Mixter, now, the thick Mixter. And I'll switch to thie big Mixter now, just use the nerve stim here. Okay. So, let's just follow that down a little bit.
CHAPTER 6
All right, so that's the accessory. So we're going to start mobilizing level Vb here from lateral to medial. LigaSure. So now, we're going to do a bunch of 2-0 ligatures, here. The reason we're tying everything here is to avoid any seromas or fluid buildups afterwards. And then, obviously, the tumor's gonna be very close to the thoracic duct, as we get into level IV here, so, we're going to have to deal with that, as well. And we're gonna sacrifice some superficial transverse cervical branches, here. This is all tumor down here. So just carve here, a little bit, like so. So, Rob, just take that for a second. Just score this here a little bit. Okay there's more tumor. Wow, he's got a lot of tumor, this guy. Bovie. All right, we'll get back to that, okay. So you can relax there, always 90 degrees to each other. Thank you. All right, so I want to see that accessory there. LigaSure. Lots of tumor. Definitely extending into level V there. Rob, just take that for a second here. Just carve here a little bit. Yep. Okay. So that's where we sacrificed the omohyoid, and then that's the other side of the omo there, okay? Come there. Take that up and show me. Just grab it big and then we're gonna tie it. Another one, please. I'll take a regular Mixter now. So I want to see that accessory. So accessory is right down there. Let me have that big Mixter, now. I'll take a LigaSure. Finally it's getting a little softer here, so that's good. That's a vessel. We're gonna preserve that. So that's heading down here, right? LigaSure. All right, so that's all stuck there, so you guys switch, now. Okay, you feel the tumor there, it's, like, rock hard. All right, so... That's good, though. So, we can... Making progress. I'm going to have to probably sacrifice the omo on that side, as well. Come through? Yep. Okay. All right. Kind of goes down there. Okay, that's clearly cancer, that lymph node too. Gently gonna bring that up. LigaSure. Okay, so that's tumor here. Just follow that vessel down a little bit. Might have to ligate that too actually. So let's just look above here, I want to see the foramen and all that stuff. I think we're gonna ligate that here. Let's tile the table a little bit more towards Nina. Scissors. Tile the table, left side up. 2-0. Relax on your right hand. LigaSure. 2-0. LigaSure. Okay. Yep, this is - that's part of the vessel. All right, have another, uh, Allis, for me. See if we can elevate this a little bit more. Just Metz that up a bit. Scissors. Just pick up the other side. Okay. 2-0. I'm gonna have a blunt tonsil. Let's hold that there for a second. Okay. Scissors. 2-0. Scissors. We're gonna get there, but that's tumor right there. That's muscle. Let's take a nerve stimy to her. See if you can find the phrenic. Should be able to take this down. 2-0. IJ is right there. Okay, see if we can get this up. That would be helpful. Light us up. LigaSure. All right, that's actually quite good. So now, we're below the IJ, here. So, this is all tumor, but the IJ is free here. And then free here, okay, so that's good. That's a blow for freedom. Okay, now you can relax a little bit here. Keep that straight, though, you don't need to pull hard. All right. Nerve stim. I'm touching something - Okay. You were just a little bit deep, there. Okay, just follow it down. It's down there, right? Well... Well, which one is it, then? That one. Okay. Okay, so the tumor is sitting right on the phrenic - Let me just see one thing. Okay, alright, that's good, though. LigaSure. We're in better shape now because we got that very lowest level IV lesion up in the air here. Okay, so... Just follow that phrenic down a little bit further. I'll take the scissors back, please, and the DeBakey. Let's see if we can put you in a little deeper, there. Have a nerve stimy to me. Nerve stimy. Okay, I think that's as low as you need to go. Okay, so that's the phrenic nerve. And we're below the tumor here, so that means we can come, come across all this stuff here. Now we're going to get close to the thoracic duct, here. So, we're going to make sure we ligate everything here. LigaSure. 2-0. 2-0. 2-0. Yep, just follow that south a little bit. So now we just have to mobilize the whole level V and now we're bringing it medially. We've got the greater auricular here, we've got the accessory up here, and the phrenic down here, so we know this is all safe. And then soon we're going to bring that whole specimen from lateral to medial. Let's hold that up north for a second. Nerve Stimy. Okay, that's the phrenic. 2-0. Bovie. Okay, that's the tumor, yep. We'll just push that tumor down there. Just hold that north there, so the phrenic heading up there. Okay, right there is good. Hold tension there. Yep. You got it. Okay. Then just Metz on those two. Scissors. Okay. That's pretty good, so we're going to flip it now. So now, we're mobilizing the whole specimen from lateral to medial. I want you to score along the sternocleidomastoid, here. I need a good, uh, Mixter or something. Don't need to go bananas there, so just... That's good. Okay. That's good. You take this now. So now, we're going as high up here in level II, identifying the med - hypoglossal again, that we dissected out before. Take a Bovie, now, actually. Bovie. DeBakey. Oh yeah, let's just do this. So, LigaSure All right. Bovie. All right, let me take that for a second. I just think you can just carve it now. Let's just see below, here. Can you bring that up, this lesion? That's the IJ from below, here. I think just divide that and see what happens. Here? All right, is it just better to take all that with us? Over to the right, right there it's pretty hard. Over here if I - Hmm. I think if I divide on top, there's a soft spot here. Yeah, I think if I come through here... Yeah, yeah, so try that, yep. Okay, okay. Can you bring that more towards you? Carve that open. So, you hold for me. You hold for me, I'll tie. You know, let's have this... I'll take an Allis now. Gonna take this muscle with us, yep. Just Metz that. Scissors. Hold tension. LigaSure. Yep, tie that. All right, heavy scissors to me. Just hold that there. This will - first will go in level III. Level III? Yeah, and this level II. All right, so now, our IJ is a little bit more free, here. Take a squirt. And have a Ray-Tech up. Take the pickups. DeBakey. Bovie. It's just scarred in here from the previous operation. Okay, that's good, so now, the question is can you carve out the vagus a little bit better? And the IJ. Oh, that feels like tumor there, okay. All right, so follow the vagus nerve. I think you can make it come through all that stuff. So, let's bring that up, and then, are we free here? Not yet, huh? Okay. All right, let me have a couple of Allises and then a blunt tonsil. So, where's phrenic? Phrenic's down there. Carotid down there. All right, so now... Can I have a blunt tonsil and then a big Mixter, now? So now, we're just going to follow the common carotid down here. Staying away from the nerve. The vagus, that is. All right. But, you know, the tumor extends all the way down here, so if we have to sacrifice this, we'll have to... All right, so, that's good. I think we're gonna ligate it here, ligate it below, So, but you guys switch now. That's still omohyoid, okay. Can I have a couple of 2-0 silk, I mean 3-0 silk popoffs? We're gonna do both. So, shine down here, that's the phrenic. All right, that goes in level IV. Level IV. Pull a bit harder with that hand. Okay. You know what... Just let that hang. You don't need to take it out, ju st let it hang there. I just want to make sure we're not getting the vagus up there. Okay. Pickups. You want me to pull the IJ towards me, so you can...? No, I just want to - I think we need to mobilize this, right? That's a branch. Take another one. 3-0. Yeah, because all this here is tumor, so that IJ definitely needs to go. So let's do this - we're gonna ligate this here. Now scissors, and 2-0 duo. Okay, so I'm just gonna do that. And then a 3-0 silk popoff. Scissors to me. 3-0 silk. I'll take a 2-0. 2-0. So I'll tie, you hold tension towards you, and then you can LigaSure that side. So follow the vagus down. Blunt tonsil to Nina, yeah, that's gonna be a vessel- I think that's gonna be a branch in there. All right, take a couple of Allises. Let's put the Allis here. It's pretty stuck here. Pickups, Mixter. Can I have a fine Mixter. Gee, that's all tumor here, huh? But this is the vagus below, right? Uh, just follow that. Yeah, I think you're just gonna have to go for it here. Just get this down first, yep, yep, all the way down. All right, let's see if we can get around it below. Just follow it south there. Okay, that's good. All right, so where's our IJ now? Okay. You have another yellow vessel loop? It's all stuck here, okay. That's tumor too, okay. All right, let's leave this here for a second. And I'll be around the IJ below there now. I should be, right? So, we have this. This is not around the IJ, this is just - Yeah, okay so let's take that first, because it's clearly not vagus, so, let me just set this up so we can see. Hold on, uh, just want to... Okay, so you can... A Bovie to me. Scissors. I need you to crank that pretty hard, there. Okay. 2-0. All right. So now, this is the, this is the IJ. I'll take another 2. So, we're going to doubly ligate this, too. So, I'm going to help you down, all the way down there. That it? Right there is good. This is just specimens, now. You don't suture ligate? Below, yeah... Still feels hard underneath it. But we'll be able to get to that though. All right, 3-0 silk popoff. All right, down here it's softer, so we're getting below it, now. DeBakey, please. DeBakey. So, we're ligating the internal jugular vein here because it's involved with the cancer. Again, the yellow vessel loops are on the vagus nerve. That's very adherent to the cancer, as well. 2-0. Hold on, just get - slide that south. Just put that with level IV, okay. Yep, there's going to be more. Gee, this is rock hard, here. We're making progress, though. All right, uh, have another blunt to me. You know what? I think we're going to have to carve it off the vagus from here. I'll take the scissors, please. All right. All right, so I'm going to hold tension here. Yep. Yep. Yep, don't worry about bleeding, just cut through it. Yep. Yep, yep, yep, yep, yep. Okay. Okay. So, we're going to send a specimen, going to - for permanent, it's going to be called left vagus nerve margin. For permanent. Left vagus nerve margin. Okay. That's left vagus nerve margin. There's going to be a little bit more. Can I have another DeBakey, please? DeBakey. Okay. All right, that seems like it's... All right, so now, finally, the vagus is free here. So now we've got the vagus cleared, all the tumor. We ligated the IJ already. We've got the phrenic down here, so now... And where's our... Okay. So now, we can come back and take it from above. Okay. All right, I'll have that big Mixter, now. And a 2-0 tie, please. Oh, not easy, not easy, not easy. I think the vagus is going to be okay, though, actually. I question whether to resect it altogether, but, you know, I think that's - that's a lot of morbidity, with unclear benefits, so... 2-0. LigaSure. Scissors. Pickups. Here's our carotid, here. Okay, so get right on the carotid. Yeah, this is tumor too, though, right? We're gonna take that separately, I guess we can, right? Yeah, tumor's like wrapped around every structure. Yeah, wrapped around the carotid, yeah. All right, so I'm gonna take this. All right, scissors to me. Just follow the carotid down there. Okay. 2-0. Yeah, the cancer is stuck to the carotid too. You don't need to pull very hard, but keep that deep. All right, I think... These are level IV. Okay. I think you just carve this here, see what happens. Bovie. Just going to protect the carotid, here, and then, so stay below - you see the tumor, so this is tumor, so I want to stay below that. Yep. Okay, let's take a look. Okay. Yep, don't worry about that. All right, finally, uh! Not easy, not easy. All right, heavy scissors to me. Take that. This is level V. Level V. That's level IV. Level IV. And then some more level III. And level III. Okay, all right, I'll take a squirt. That's going to buy him at least 5 years, you know? All right, carve that out. Bovie. Oh, I got it here. Just this little piece? Yeah, let's see, is that... That's - Okay. That's just... This is - goes in level IV, too. Level IV. He's got a good chance of having a surgical cure with this operation, you know? Level IV. Level IV. 3-0 tie. Scissors. I'll have a fine Mixter, and then a 3-0. I'll take another squirt.
CHAPTER 7
All right, so, here is the vagus nerve that we preserved, that was very adhered to the tumor. Uh, take a pickups to me. We ligated the internal jugular vein down here. Here is the IJ, uh, ligated below and above. This is the vagus, which we preserved, even though it was very adherent to the nerve. This is the, uh, common carotid artery, as well as the carotid bifurcation, which we preserved. And up here is the hypoglossal nerve. 3-0. Can I have the nerve stimulator? Scissors. So here is the hypoglossal nerve. Here is the phrenic nerve. Hypoglossal and phrenic, okay. So, this is the greater auricular nerve that we preserved. It's right up here. And that's the spinal accessory nerve there. All right, give us a Valsalva, now, to 40. That's the omohyoid. Yeah, that looks good, all right. So, we can take this off. So, you can- We're going to run around, so tilt to table the other way now.
CHAPTER 8
All right, so now we're over on the uh, right side. So based on preoperative me- Based on preoperative imaging, it doesn't have as extensive disease, but certainly biopsy-proven disease on this side, as well. So again, the same thing, we're identifying the greater auricular nerve first. Take another double skin. So, crank that, really hard. It's like still not in there. Okie dokie, that's good, so let's take a thyroid retractor now so hold that. Good? Yep, that's good. Yeah, just stay superficial. Okay, go up to that. Yep, open that up. Just opening the lateral border of the SCM, here. All right, that's good, so let's go find the spinal accessory. This you can just carve here. All right, that's the nerve right there. All right, I'll have an Allis to me now. All right, I'll have a 2-0 ligature now. Okay. Yeah, I think anesthesia wants to steal the show a little bit. That's why they did that thing with the hiccup in the beginning, you know. I'm just saying that you guys wanted to be, sort of, part of the show and steal the show. That's why you did that - That's why you did that hiccup, so you could be... Focal point. Yeah, the focal point, the center piece. Yeah, I told her to go brush her hair. I would have put lipstick on beforehand. Okay, I'll take a thyroid retractor, now. And take another Allis.
CHAPTER 9
All right, show me that nerve again. Okay, so it's heading down there. Okay, let me have the big Mixter, now. You can do a little scoring here first. Just score along there. 2-0. 2-0 tie. All right, so I'm just going to put you in a little deeper, there. Liggy. Scissors. Yeah, let's see... I'll take a squirt. All right, so Rob, just take that for a second. Just carve this here. 2-0. All right, that's good for now. All right, so, next order of business, we're going to dissect out the sternocleidomastoid muscle. So, we're going to open up the medial border first. I'll take a blunt tonsil, now. So, Rob, take that. So advance this. Stay high up here. Rob just take that for a second. Okay, so follow that up. And touch me. All right, we'll take a large Penrose. Kelly. Okay, and then... You can get lower now. Okay. Okay, that's pretty good, all right. Okay. So, slide that laterally. All right, so this is the omohyoid. So, on this side, in contrast to the left side, on the right side here, the omohyoid is not involved with cancer, so we're going to be able to preserve the omohyoid, here. Just touch me here. All right, I'll take a small Penrose. All right, I'll take that from you. DeBakey. Okay. Have an, uh, have the big Mixter, now. 2-0 tie. I'll take a LigaSure. 2-0. Okay, so we'll come back to that. Just hold those.
CHAPTER 10
All right, so next, we're going to dissect out IJ and the vagus. Pickups, blunt tonsil. So the tumor, I'm feeling the tumor sitting right here. Take a feel there, Nina. Take a feel there. All right, so bring all that over towards you... All right, we'll take a blue vessel loop next. Let's see - let me have that. Can I have a DeBakey, please? 3-0 tie, please. I'll take a squirt. Scissors. Okay. Take a Bovie, carve that there. Yellow vessel loop, please. Okay. All right, that's pretty good, right? So that's really as high as we need to go.
CHAPTER 11
This is level II. So just, just right underneath it. So just this? Yep, yep. And then go a little deeper. Yep, right here. And just carve all this stuff. Yep, don't go too deep there. Okay. Yep, just amputate there. Yep. This is level II. Level II. 3-0 tie, please. So that's right modified radical neck dissection level II. You got it, right Rob? Yeah. Okay, so then, you come below now. Okay, so take a blunt tonsil to her now. Mixter now, pickups. Yep. Keep it there. And angle towards you a little bit more. Get this little bend here just on top of the vagus. Okay, that's good. So, let's start laterally, then. Take those out. Okay, we'll take a couple of Allises, and a blunt tonsil, now. So now, again, we're starting to mobilize things from level V, following the accessory. So, LigaSure to me. And mobilizing all the level Vb lymph nodes here. 2-0. 2-0. All right, we'll take the nerve stimmy next. Yep, that's the phrenic right there, right? Pickups. 2-0. All right, so I'll tie that. 2-0. So, I'm just going to put you deep here. So, you're holding the IJ, so, be firm, but gentle, okay? Bovie. This is all tumor, here, but, in contrast to the other side, it's coming off easily off the omohyoid muscle, as well as the jugular vein and the vagus nerve. So it's clearly free, there. Then we have the phrenic nerve down here. Just stimulate the phrenic again as it's heading up there. Okay. I'll just take a Bovie now. Okay, so just swing that. So now we're going to bring the whole specimen from lateral to medial, here. So, we've got that. Then just take that. All right, so I'll take a couple of Allises. All right, so, let's follow that muscle now. What is that? What, uh, something was beeping there? No? You want to bring that over. I think the GoPro is low on battery. 2-0. LigaSure. So, just carve this out, now. Pickups. Okay, so just score that north. Bovie. Score that. Tumor there. Uh, I think that's just a normal lymph node, but - No, no, it's, that's a lymph node, but I don't think it's - Oh, maybe. Let's see. I'll have a blunt tonsil for a second. This is stuck there. I'll have the fine Mixter, now. That's level II. 2-0. Just keep that towed in, like so. You got it? All right, so we got phrenic down there. Just gonna hold the vagus like so. Yeah, I think you can just carve here, see what happens. Because here's the vagus, here's the carotid, so you take that now, and we can Metz the vagus off here. Just put that here. Okay. Let's see. You can relax up top now. 2-0. Dr. Carling, I'll be right back. Okay. Close here? Closer. Ligy. LigaSure. Scissors. So, always 90 degrees. You're going to hold the IJ again. So, uh, he'll hold that. So stay right there. Got it? That's phrenic, there, so stay right - Just take Bovie, here. Okay. Scissors. 2-0. 2-0. 2-0. 2-0. Okay. All right, so that's the specimen. So take heavy scissors, now. DeBakey. I'll take that. So, take a feel here. So this is the whole, the big tumor there, on that side. Heavy scissors. Okay, so this is level V. Move your finger. I think you may have the buckets already. Right modified radical neck dissection level V. Here's level II. Level II, there's already some stuff in it. This is level II? That's level II in your hand. This is level II. He should, he already started putting stuff in level II. We're going to start closing here, very soon. This is level III. Level III. And this is level IV. Okay.
CHAPTER 12
Level IV. All right, I'll take a squirt. Take a Valsalva to 40. All right, we can come down. All right, so we have the vagus nerve here, nicely dissected out. I'll take the nerve stim. And then... Pickup. It's underneath here. That's the phrenic nerve. Yep. And then, so here's the carotid, which was not as involved as compared to the other side. The carotid bifurcation. The IJ. Controlled with a vessel loop. And then, show us the accessory - Put that back in. That's the accessory. Nice. All right, give us one more Valsalva. Put that in there. Are you doing it? That's the greater auricular nerve. Looks nice. Okay. You got too much? All right, you can come down. 2-0. We're going to use 2 drains, #10 flat JP. And drain stitches. So, we didn't need to go as high, but the digastric is right here.
CHAPTER 13
Okay. And then I'll have the table down a little bit. Okay, that's good. Make your holes, now. Drain. Let's take a look. Drain. No, the drain. Heavy scissors to me. Well, let's, let's look at this over here first. So, tilt the head towards you. All right, give us a Valsalva. All right, give us a Valsalva now, squirt. All right, do it one more time. All right, cut the needle. Cut the needle. Cut the needle - okay, too late. Here's the needle back. Hold this. 3-0 Vicryl. Adson.
CHAPTER 14
Three.
CHAPTER 15
So, as you could see during the operation, we started on the left side, doing the left modified, uh, radical neck dissection. And, uh, there was obvious, uh, invasion of the tumor in the, uh, left level IV lymph node compartment, into the internal jugular vein. So, as you could see during the operation, I sacrificed the vein. And it was also very adhered to the left vagus nerve. Uh, we were able to preserve the vagus nerve, but we did send off, uh, specific surgical margins, as we peeled cancer off, uh, the vagus nerve. Uh, the right side, in contrast, was quite straightforward, uh, with some obvious bulky disease, but no, uh, extranodal extension was identified, and the, uh, operation was quite, quite straightforward. So, postoperatively, this patient will now extubate. He will go to the regular floor. Uh, we put 2 drains in, 2 number flat JPs on each side, mainly to make sure he doesn't develop a chyle leak or a seroma. We'll probably remove that on postoperative day, uh, 2. He, uh - typically, patients spend either 1 night or 2 nights. Because we did a bilateral dissection on him, he'll most likely stay 2 nights. We'll have him work with physical therapy for range of motion of his neck muscles, starting tomorrow. Initially, we start him on a low-fat diet, to make sure he doesn't have a chyle leak. Uh, postoperatively, he can continue physical therapy as an outpatient. And, dependent on what the final pathology, uh, demonstrates, he may or may not need repeat radioactive iodine treatment.