
Endolymphatic Sac Decompression
Main Text
Table of Contents
Endolymphatic sac (ELS) decompression can be performed for patients with Meniere’s disease who have failed conservative treatment such as dietary changes and medical therapy. The full pathophysiological mechanisms that result in Meniere’s disease are not entirely understood. The variation in techniques for performing ELS decompression support this; there is no concrete data to justify one approach over another. Regardless, in the correct patient, ELS decompression can significantly alleviate the patient’s symptoms. To do so, a mastoidectomy is performed to expose the bony labyrinth as well as the bone overlying the sigmoid sinus. Decompression of the sac can be accomplished by removing overlying bone, incising the dura, or stenting the dura open.
The clinical symptoms of Meniere’s disease include fluctuating-progressive hearing loss, episodic vertigo, tinnitus, and aural fullness.1 These symptoms are thought to be a result of increased endolymphatic fluid, which distorts the membranous labyrinth, though the exact mechanisms of such are poorly understood.
In this case, a 68-year-old patient presented with vertigo episodes associated with fullness and pressure in the left ear, as well as tinnitus and decreased hearing. He had attempted dietary changes as well as medical treatment with a diuretic and oral steroids. Although oral steroids made improvements in hearing, these dosages could not be maintained safely. He also had several rounds of steroid injections into the middle ear space that provided slight improvement in his hearing and relief of his vertigo episodes. Over several years, however, his symptoms became resistant to steroid injections as well as short courses of oral steroids. He also developed symptoms related to the right ear.
There were no abnormal findings on his otoscopic exam. His tympanic membrane was normal in appearance without evidence of retraction or middle ear effusion.
Vestibular testing demonstrated abnormal findings on his vestibular-evoked myogenic potentials (VEMP). His ocular VEMP responses are present but with amplitude asymmetry that is worse in the left ear. His audiogram at presentation shows that tympanometry is normal bilaterally and that his left ear has moderate to moderate-severe sensorineural hearing loss with a speech reception threshold of 55 dB and a speech discrimination of 56% (Fig. 1). After a year of symptom fluctuation and treatment with steroids (both oral and intratympanic) and diuretics, his audiogram revealed bilateral moderate-severe sensorineural hearing loss (slightly worse in the lower frequencies) with a speech reception threshold of 55 dB in the right ear and 60 dB in the left ear and speech discrimination of 76% in the right ear and 64% in the left ear (Fig. 2).
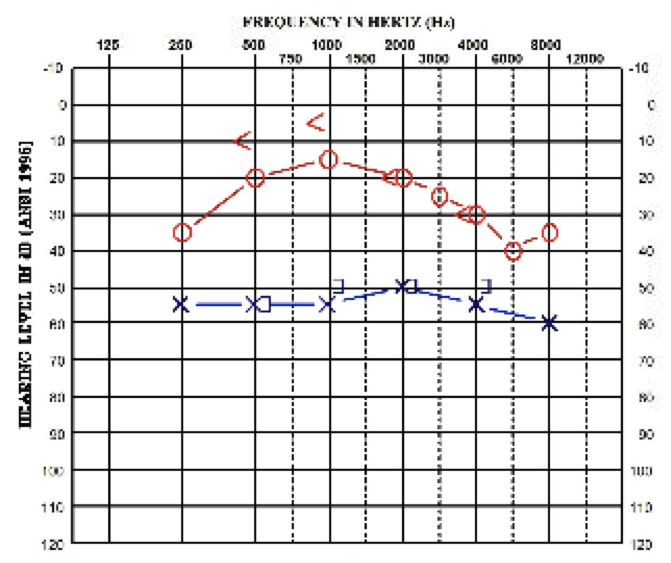 Fig. 1, Audiogram at presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue.
Fig. 1, Audiogram at presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue.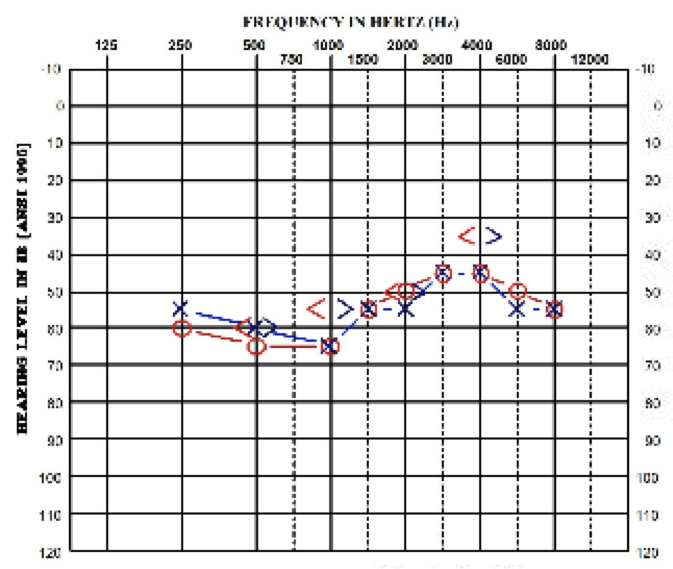 Fig. 2, Audiogram one year after presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue.
Fig. 2, Audiogram one year after presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue. Meniere’s disease may be difficult to diagnose due to the fluctuating nature of symptoms as well as the lack of any definitive testing for diagnosis. It has an episodic course, and certain patients may undergo spontaneous remission of their vertigo.2 Although the hearing loss in Meniere’s disease is typically described as fluctuating, there may also be a gradual overall decline in a patient’s hearing levels, even in the absence of other symptoms such as aural fullness or vertigo. Overall, prolonged disease may cause deterioration of hearing, and intense tinnitus is more often seen in the later stages of the disease.3
Surgery for Meniere’s disease is typically not the first option or course of treatment, and there are multiple surgical methods that can be performed. To understand the possible treatment modalities, it is important to grasp the underlying pathophysiology of the condition. The hydropic state of the inner ear has been confirmed in temporal bone studies and is described as the primary pathologic mechanism in Meniere’s disease.4 Therefore, treatments will target pathways that can influence the degree of hydrops that is present.
At the least invasive end of the spectrum, dietary changes such as the reduction or restriction of caffeine, alcohol, and salt can be implemented. In terms of medical therapy, diuretic therapy with Dyazide (triamterene and hydrochlorothiazide) can be used to decrease vestibular symptoms.5 Dietary changes and diuretics can be used for prophylaxis, while vestibulosuppressants such as valium can be used to alleviate symptoms during a Meniere’s attack. The injection of medications via the tympanic membrane into the middle ear space can also affect Meniere’s symptoms. Gentamicin, an aminoglycoside antibiotic, can be used to reduce the production of endolymph, but it has an associated risk of hearing loss.1 Intratympanic perfusion of dexamethasone contributes to the reduction of the intensity of vertigo attacks, decreases the intensity of tinnitus, and improves the average hearing threshold.6
When these more conservative therapies fail, patients can proceed to more invasive and ablative options, which include endolymphatic sac (ELS) decompression, labyrinthectomy, and vestibular neurectomy. ELS decompression offers the opportunity to preserve hearing, while labyrinthectomy and vestibular neurectomy will destroy any residual hearing in the affected ear.
This patient had been followed for several years for his condition and was only referred for a second opinion of management due to the inability of conservative management to continue to control his symptoms. Dietary changes and diuretic therapy had little impact. Initially he responded well to short courses of oral steroids and to several rounds of intratympanic steroid administration, but ultimately his symptoms persisted and proved debilitating.
Although ELS decompression carries with it the expectation of preserved hearing due to the surgical approach, there remains a risk of hearing loss with the procedure. If the patient did not have serviceable hearing in the contralateral ear, one would likely not operate on an individual’s “only-hearing ear.”
While hearing preservation is a key component of performing this particular approach to the vestibular system, the primary indication for surgery is ongoing episodic vertigo despite appropriate medical treatment. Although the pathophysiology was not clear at the time, the first surgical procedure to treat Meniere’s disease was performed in 1927. Portmann made a small incision to open the ELS in an attempt to decrease endolymphatic pressure.7 In 1962, a subarachnoid shunt to drain endolymphatic hydrops was described by William House.8
There are numerous reports regarding various techniques and materials used for the procedure, each describing improvements in hearing, vertigo episodes, or quality of life.9-11 In 2014, Sood et al. performed a meta-analysis regarding the current techniques and their efficacy for controlling vertigo and maintaining hearing.12 They found that both decompression alone as well as shunting into the mastoid cavity resulted in effective vertigo control for both the short term (12–24 months) and the long term (greater than 24 months) in patients who had no success with medical therapy. Even with newer techniques such as endolymphatic duct blockage, ELS surgery remains an excellent non-destructive surgical option for patients with symptoms of incapacitating endolymphatic hydrops.13
We used a Silastic sheet (Dow Corning, Midland, Michigan, USA).
Author C. Scott Brown also works as editor of the Otolaryngology section of the Journal of Medical Insight.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Packer MD, Welling DB. Surgery of the endolymphatic sac. In: Brackmann D, Shelton C, Arriaga MA, eds. Otologic Surgery. 3rd ed. Philadelphia, PA: Saunders; 2010:411-428.
- Silverstein H, Smouha E, Jones R. Natural history vs. surgery for Meniere's disease. Otolaryngol Head Neck Surg. 1989;100(1):6-16. doi:10.1177/019459988910000102.
- Havia M, Kentala E, Pyykkö I. Hearing loss and tinnitus in Meniere's disease. Auris Nasus Larynx. 2002;29(2):115-119. doi:10.1016/S0385-8146(01)00142-0.
- Okuno T, Sando I. Localization, frequency, and severity of endolymphatic hydrops and the pathology of the labyrinthine membrane in Meniere's disease. Ann Otol Rhinol Laryngol. 1987;96(4):438-445. doi:10.1177/000348948709600418.
- van Deelen GW, Huizing EH. Use of a diuretic (Dyazide®) in the treatment of Ménière's disease: a double-blind cross-over placebo-controlled study. ORL J Otorhinolaryngol Relat Spec. 1986;48(5):287-292. doi:10.1159/000275884.
- Sanković-Babić S, Kosanović R, Ivanković Z, Babac S, Tatović M. [Intratympanic corticosteroid perfusion in the therapy of Meniere's disease]. Srp Arh Celok Lek. 2014;142(5-6):291-295. doi:10.2298/SARH1406291S.
- Portmann G. The saccus endolymphaticus and an operation for draining the same for the relief of vertigo. J Laryngol Otol. 1927;42(12):809-817. doi:10.1017/S0022215100031297.
- House WF. Subarachnoid shunt for drainage of endolymphatic hydrops. A preliminary report. Laryngoscope. 1962;72(6):713-729. doi:10.1288/00005537-196206000-00003.
- Durland WF Jr, Pyle GM, Connor NP. Endolymphatic sac decompression as a treatment for Meniere's disease. Laryngoscope. 2005;115(8):1454-1457. doi:10.1097/01.mlg.0000171017.41592.d0.
- Convert C, Franco-Vidal V, Bebear JP, Darrouzet V. Outcome-based assessment of endolymphatic sac decompression for Ménière's disease using the Ménière's disease outcome questionnaire: a review of 90 patients. Otol Neurotol. 2006;27(5):687-696. doi:10.1097/01.mao.0000227661.52760.f1.
- Kim SH, Ko SH, Ahn SH, Hong JM, Lee WS. Significance of the development of the inner ear third window effect after endolymphatic sac surgery in Ménière disease patients. Laryngoscope. 2012;122(8):1838-1843. doi:10.1002/lary.23332.
- Sood AJ, Lambert PR, Nguyen SA, Meyer TA. Endolymphatic sac surgery for Ménière's disease: a systematic review and meta-analysis. Otol Neurotol. 2014;35(6):1033-1045. doi:10.1097/MAO.0000000000000324.
- Garcia MLF, Segura CL, Lesser JCC, Pianese CP. Endolymphatic sac surgery for Ménière's disease – current opinion and literature review. Int Arch Otorhinolaryngol. 2017;21(2):179-183. doi:https://doi.org/10.1055/s-0037-1599276.
Cite this article
C. Scott Brown, MD, Calhoun D. Cunningham III, MD. Endolymphatic sac decompression. J Med Insight. 2023;2023(202). https://doi.org/10.24296/jomi/202Procedure Outline
Table of Contents
- Anesthesia
- The surgery is performed under general anesthesia.
- The endotracheal tube should be secured to the patient’s mandible on the side opposite of the planned surgery.
- Perioperative antibiotics should be administered within one hour of the incision.
- Because facial nerve monitoring is used, the patient should not be paralyzed during the procedure.
- Patient Positioning
- The patient will be rotated 180 degrees with the head opposite of anesthesia.
- The patient is laid supine on the operating table, and straps are placed after tucking the arms so that the table can be rotated with the patient secured. A shoulder roll is not required. The patient’s head should be rotated to the opposite side so that the mastoid is parallel to the floor.
- Facial Nerve Monitoring
- Ground and stimulation electrodes are placed in the subcutaneous tissue overlying the sternum.
- The orbicularis oculi and the orbicularis oris muscles are monitored by placing ipsilateral electrodes into these muscles.
- Prepping the Patient
- The patient’s skin behind the ear is cleaned with an alcohol solution after any hair overlying the postauricular area is shaved.
- Mastisol is applied in four quadrants surrounding the ear, and adhesive drapes are applied to block out the ear and mastoid.
- A cotton ball is placed in the external auditory canal, and the area is prepped with Betadine solution.
- Four sterile towels are used to block out the area, and a split drape is placed. A single Ioban drape is placed over the field.
- Local Anesthetic Injection
- A C-shaped postauricular incision should be drawn with a marking pen approximately 1 cm posterior to the sulcus. Several perpendicular lines may be drawn with the marker to help reapproximate the skin during closure.
- The skin and subcutaneous tissue should be infiltrated with local anesthetic consisting of 1% lidocaine with epinephrine in a concentration of 1:100,000.
- Approximately 5–10 minutes should pass to allow for the vasoconstrictive properties of the epinephrine to take effect.
- Incision
- The incision should be carried through the skin and the subcutaneous tissue to a plane just superficial to the temporalis fascia. This should be performed inferiorly towards the mastoid tip and superiorly above the temporal line.
- With the muscle exposed, the subcutaneous tissue can be retracted with a self-retaining retractor.
- Subperiosteal Flap
- The mastoid muscle-periosteal layer should then be incised in a “7-fashion” through the muscle and directly onto the bone using monopolar cauterization. Care should be taken inferiorly to palpate for the mastoid tip to ensure that the instrument is not plunged more deeply.
- An anterior based muscle-periosteal flap can then be elevated using a Lempert elevator to expose the posterior bony ear canal and the mastoid cortex.
- The linea temporalis should be exposed superiorly to help approximate the level of the tegmen mastoideum.
- The sterile operating microscope should be brought into the field in order to facilitate microdissection.
- With a 5-mm cutting burr on the drill, an intact canal wall mastoidectomy should be performed down to the level of the antrum and the horizontal semicircular canal. The dissection should begin superiorly near the temporal line to help demarcate the superior limit of the dissection.
- The cortical mastoidectomy should be carried inferiorly directly behind the bony ear canal. The cortical bone is removed and widely saucerized with the deepest level of the dissection in the anterosuperior quadrant below McEwan’s triangle.
- When the antrum is reached, the cutting burr should be exchanged for a diamond burr to facilitate more cautious dissection. With this in place, the horizontal semicircular canal, sigmoid sinus, and tegmen mastoideum can be dissected.
- After thinning the posterior external auditory canal, the facial nerve can be identified just distal to the second genu as it turns into the vertical mastoid segment. A thin layer of bone should be left along the course of the facial nerve.
- The bone overlying the sigmoid sinus and posterior fossa dural plate are thinned by removing the retrofacial air cells.
- When looking for the endolymphatic sac (ELS), consider Donaldson’s line, an imaginary line that can be drawn along the horizontal semicircular canal that bisects the posterior semicircular canal. In the area where this line meets the sigmoid sinus, the ELS can be estimated just anterior and inferior to this junction.
- As the bone in this area is removed, note a thickened area of the posterior fossa dura that denotes the sac. When the bone is compressed, gently pressing on the sac may reveal the duct running anterolaterally as it tents the dura in the direction of the posterior canal.
- With the ELS completely exposed, the sac should be opened using a sickle knife along the posterolateral aspect.
- Shaping the Stent
- A T-shaped stent is fashioned from a Silastic sheet.
- Placement of Stent
- The upper part of the “T” is folded onto itself and placed within the sac, so that in trying to unfurl itself, it stents the lateral layer of the sac open.
- A piece of Gelfoam is placed over the surgical site.
- The periosteal layer is closed in interrupted fashion with a 3-0 Biosyn suture. The corner of the “7-incision” is brought together first, followed by the other areas. This does not need to be a watertight closure, but this layer should be well-approximated.
- Using the same 3-0 Biosyn suture, the subcutaneous layer is also closed. This is performed with deep interrupted suture to bury the knot, while reapproximating the skin edge.
- A thin layer of Steri-Strips should be placed along the length of the incision.
- A House-mastoid dressing should be fashioned from 4x4 gauze. This dressing is placed over the ear and mastoid being operated on, and secured around the head using two inch Kling roll gauze. Care should be taken to ensure that this dressing goes below the occiput to help prevent it from sliding off of the vertex. This dressing is left in place for 24 hours and removed at home.
- Patients are discharged on the day of surgery.
- Postoperative Restrictions
- The patient is sent home on a week of antibiotics (Keflex). They are also given anti-nausea medication as well as pain medication (Norco).
- They are advised to perform no heavy lifting (greater than 8–10 pounds) for 2–3 weeks after surgery.
- They are seen 3 weeks after surgery to assess the wound, and an audiogram is obtained at three months to reassess hearing outcomes.
Transcription
CHAPTER 1
So this patient is a 69-year-old malewith intractable left-sided Meniere's disease.He has failed multiple medical regimens,including diuretic therapy, low sodium diet, as wellas both oral and intratympanic steroid injections.He’s continued to have debilitatingepisodes of vertigo.These are classic rotary vertigo symptoms lasting two to three hours,and so he does still have usable hearing in this left ear, which is fluctuating.And today we're going to be doing atransmastoid endolymphatic shunt procedure.Can I have the injection, please?The 1:100,000.
There are various philosophies about the shunt surgery.There are some surgeons who prefer not to doshunt surgery at all, as they do not feel that itis that beneficial,whereas some surgeons prefer to just decompress the endolymphatic sacand the surrounding dura.And then the other option is to actually placea stent or shunt into the lumen of the sac, which is what we'regoing to be doing today.I prefer to use a T-shaped stent, which ismade of .005 inch silastic, and that's something we will fabricate here in the ORprior to placing it.We use a standard postauricular incision for doing this surgery.And 15 blade.
We’ll make a postauricular incision a little bit smaller than a standardpostauricular incision.We don't need quite as wide exposure as we would need ifwe were trying to turn the ear forward to get into the ear canal.Okay.And we'll carry this incision all the way down to the muscle periosteal layer superiorly.Can I have a bipolar, please?Okay, can I have a Bovie now?Actually a large self-retaining retractor first.And the Bovie.Oops, sorry.Mm hmm.Oh, sorry - I didn’t mean to...Make it so difficult.So we are going to score the muscle periosteal layer in a 7-fashionjust to create a muscle periosteal flap and expose the mastoid cortex.Lempert elevator, please.
Okay.And we’ll take this muscle periosteal flap just to the posterior edgeof the external auditory canal.So we have the entire mastoidexposed now.The spine of Henle can be seen anteriorly here and the mastoid tip.We're going to begin with doing a cortical mastoidectomy,and we will - our primarygoal is to identify the lateral semicircular canal,and antrum, and the sigmoid sinus.The endolymphatic sac often is located in an area - if you draw aline tangentially along the lateral semicircular canalwhere it meets the sigmoid sinus justbelow and anterior to that line, is typically the area of the endolymphatic sac.And that is known as Donaldson's line.May I have the suction, please?And then two folded towels and two Allis clamps.
CHAPTER 2
Number 4 - fluted burr, but it's a pie burr.Do you have a Gimmick?Focus like right in here.Right in this area, right here.All the way back posteriorly - we got to find the sigmoid.Good. All right - keep going.Go through all that - that’s all air cells.And that must all -Koerner's septum below you.Now you can open up a little bit more down there.Mm hmm.Okay, let's get down to antrum.One thing you want totry to avoid is doing this - you want to try to avoid doing - like you want tokind of get your suction set up somewhere and then never move it,and just on and off kind of doing like that.Mm hmm.And thin that posterior canal wall.All that bone to your left - all that Koerner's septum - all the way back -saucerize it.Mm hmm.Mm hmm.Good.No, he’s going home.Just keep going.So we don’t need to get too far anterior because we don’t want toopen the antrum too much because you get a lot of bone dustgoing in there, and sometimes it'll fixate the ossicular chain.Yep.Mm hmm.That’s probably mast- give me a second.Mm hmm.Direct a little more superiorly there. Yeah,come - shift to your left, so you're looking up high.Okay, and thin the tegmen because actually she's got kind of a high tegmen, and we’re a little low.So don't...Just undercut it, then we'll have to take the space up here too.Mm hmm, that’s going to be the antrum, right in there.Mm hmm.Mm hmm.Okay - hey how are you doing? Good.Okay, so there’s lateral canal, right deep in there.Maybe - maybe we don’t see it quite yet. Yeah, I don’t think we do yet.Just take a little bit of that. Just kind of take this anterior ledge?Yep.Okay.Come all the way out laterally. Yep, that’s good.Mm hmm, now - wait, look and see first - it’s going to be right there.Okay.I'm just going to come back and open all this up.Yep, so now, we need to -we need to find sigmoid, but we need to kind of come back in -just focus in that area there.Okay - should I saucerize this?No, I don’t think that matters too muchbecause the area we want to be is ultimately going to be right down in there.Okay, I'm starting to feel a little sigmoid there.Right under it. Just find the sigmoid.Can we have a Bovie for a second?Okay.Just smooth out a little bit more back - kind of - go back to here.You know, because he’s got kind of a - he’s going to have a - more of a flat sigmoid.Mm hmm, okay.And try to gently thin some more of this stuff in here.Use the side of your burr - turn your - rotate your hand up.Yep.Mm hmm.All the way towards the - yep, just in there.Mm hmm, all the way out lateral now, moving on it.Mm hmm, yep.Mm hmm.Yep, just now delineate your sigmoid better.Mm hmm.His sigmoid doesn’t ride up like a big dome. It’s more of a,sort of a flat sigmoid.Mm hmm.And really we'd like to kind of decompress the top half - the anterior halfof it. We don't have to decompress the whole thing, but…So yeah, try to get some of the bone out of the sinodural angle. You know,where the sinus and the tegmen approach each other.Okay, Gimmick?So Scott, now you want to get... All this bone in between?Well no, you want to, kind of get this stuff out of here. Okay.Those are all air cells still.Now very gently come in there.Mm hmm.Let me...Yep.Take that down there?No, I want to see lateral canal better.Yeah, I agree.So open up a little bit moreof this bone right here. Okay.Thin the posterior canal wall a little bit more. Take out - did you see how thick it is?Put more up top here, focus it - yeah, right in there.Mm hmm.Yep.Mm hmm.Mm hmm.All right - hold on a second.There's that. Let's go ahead and get...Get a little suction in there now.It still looks like trabecular to bone,maybe lateral canal just under that... Right there.Right there is lateral canal.So you can come through some of this stuffhere and smooth down some of that. Okay.Mm hmm.Mm hmm.I'm starting to see it a little better underneath this little trabecula there.Mm hmm.Now just cut through this and...Mm hmm.Yep.So there’s lateral canal, so - and then here’s -if you look through - maybe it’s still lateral.I thought maybe that's posteriordown there.So one thing we can do to kind of speed things up, is just kind ofthin all this down real quick.And then all I’m wondering is - is that still part of the lateral -or just part of posterior canal?Right there.Yeah, so see - let me have a Gimmick?Water off. Let's go to a 7 suction irrigator.So the lateral canal is kind of coming like this, and then that’s posteriorcanal, running like that.And so what I want you to dois just take your diamond - let's go to a - do you have a 4 diamond?And at about that level, just start kind of thinning that. We’ll look for facial nerve.Okay.All right, yep.Yep, all the way down - use the whole length.Mm hmm.Keep going.Mm hmm.Yep, right in that level right there.You don’t let white char build up.Mm hmm.Keep going.I'm starting to see it there.I'm starting to see it there, I think - right underneath me.Unless it’s just mucosal... Well yeah, could be.Just paint a little lightly - very lightly over that area.Yeah, I think you might be right. Can’t tell yet though.I'm just trying to kind of thin the bone around it a little bit.Mm hmm.If that’s it, it’s going to be swinging up laterally.So this is one of those temporal bones where the air cells are righton the nerve. Sometimes you pop through an air cell and there’s the nerve.Yeah, I think that's it,and then there’s chorda right above it. Yeah.I think you’re right. Okay. Maybe? That’s what it looks like at least.So now decompress the sigmoid,the top of the sigmoid and kind of the front part of it.That's okay. Don't worry about it.The area you really want to be focusing is more superior on the sigmoid.So right where that lateral canal and the sigmoid meet,just below there is where we’re going to need to remove bone from.Yep, get that bleeder.Mm hmm.That’s not fossa, is it? No.Okay, come up - bring it up laterally more. You’re just below it.A little bit more.Don’t put water on - keep the water off. Water off.Yeah, hold on, I don’t - yeah, I don’t - don’t do that.Get a little bone wax there or something. Okay.I can finish opening this up here though.Yeah, just open that a little bit more inferior to where you are. Water on.Yeah, right there I am. Just sort of inferior and medial to that.Here is the dura? Yeah.
CHAPTER 3
Good. Oh, yeah.Yeah, yeah, yeah. I think maybe it's sac right there too.See how that’s real vascular?That’s a nice - a real nice look at the posterior canal. Yeah.So here is lateral semicircular canal and then posterior semicircular canal.And I think you may be - let's see, where is that?A little more water.I can't tell if that...I think I'm right about that... Yeah, I think you might be.And there's chorda coming off of it... It seems a little bit strange though.I don't know, I’m not 100%.We don’t really need to get too much...And that’s dura there, and that's just a blood vessel in the dura.And so I’m going to go aheadand decompress this sigmoid a little bit more.And we’ll actually bipolar those little vessels on that.Some people say just decompressing is also good.Yeah, he’s got a weird, really flat, sigmoid sinus.Not that that is a predictor of anything.That we know of.There’s a retrofacial air cell in here.Mm hmm. Very vascular.I'm not so sure that is facial.Now, we want to come back this way.Let's decompress just a little bit more.It's very vascular. Okay, now water off, please.Can I get a bipolar?Uh, huh.Now can I - do we have a J dissector like we had on that last case?It's right on your tray.What’s that?It's on your tray.Wonderful.Can I have that, please?I like getting this bone really thin, and then rather than drilling it away,just kind of separating the dura because I'd like to - if possible, you want tokeep this dural surface really clean, and not get it abraded too muchbecause once it gets all of ratty and kind of abraded, it getsdifficult to tell where the sac is.And so we’ll kind of just flick this bone off, and then push the dura awayfrom the bone, and that way the sac won't - look at all these blood vessels.Yeah, they're huge.Let’s have the bipolar.Well, people have talked about the vasculature, like - bipolar -these blood vessels between the sigmoid, and the sac, and the dura,and maybe, you know, maybe have something to do with it, but I don't -I don't, who knows.Mm hmm.Come on.So I usually do bipolar them all.All right now, the - the J dissector again.So then we can kind of flick some of that off,but we can also drill all that away.Mm hmm.Well, maybe. Yeah, that’s part of the sac right there.Okay, drill.Or drill.I mean I’m looking at posterior canal -here.We’ll take this right up beside the posterior canal, which is right there.Yeah, that's probably the sac.These are theretrofacial air cells that we see.Water off for a second.He’s got a lot of…Mm hmm.All right.Let’s see the control pedal.Water on.Water?You have to be cognizant of the facial nerve coming in inferiorly there, right?Yeah, the facial nerve? Yeah.The facial is up here. So there’s the level of the lateral canal.The facial is running kind of in this direction, soif we -if we kind of come up here, we can -we can kind of follow it.And you see how it’s running now.You don’t always have to find the facial nerve. I think it’s a goodidea to find the facial nerve because when you know where the nerve is,you know how far underneath it you can go. And a lot of times the sac islocated pretty - kind of far anterior down in this area here. I think we'reseeing the edge of the sac right there. So we're going to just geta little bit more of this bone, and then we’re really pretty closeto being - getting the exposure that we want.Mm hmm.Now that J dissector again.Please? Water off.So we’ll kind of push this down.Uh huh.Separate that.And that’s the sac right there.At least he’s got a pretty good sac though.You can actually see how these fibers are kindof radiating, coming back that way.So okay, drill.I'm going to take this right up to the edge of theposterior canal. Water on.So we’re just getting a little bit more anterior exposure here. Water off.J dissector.But you can see the area of the sac pretty well.See how it's real white right in there?And sigmoid is continuing to traverse downin this direction.So we can see, this is the top of the sac right here,and it kind of comes down at - like this. And if we draw a linealong the lateral canalwhere it meets the sigmoid,usually that's about the area, which is thetop of the sac.But you see - see how at it tents up right there?Do you see that Scott? Mm hmm.That’s - so this is all the sac here. We'll just get a little bit morebone, and then we're really done.He's got a good - this is a good one, so…
CHAPTER 4
Can I have a bulb irrigator?There’s the sac right there.Completely decompressed.Now we're going to fashion our stent.I’m going to take thatsilastic and on - if I can have it on a Teflon block.And I'm going to need a marking pen.And there’s no realscientific means to this.Can I have a bulb - I mean, a green towel - fresh, green towel?Silastic block.And the marking pen.So usually - man that's bright - I will mark it out a little bitfirst - just a general...Okay, now an 11 blade.I hope so.Do you have an 11 blade?So I’ll make a little line like this.And then actually,this will becut like that.And then...Are you making a capital T? Yep.All it is is a T.Have you seen that before?I had one really, really, really long, andit was a really crummy one. It was super small and tucked in. It was the oneyou ended up doing the lapendectomy on.Oh yeah.So, you can sometimes tell.Like, I don’t - like, he’s got a really good sac, so I think he will do wellbut you are correct in that some people just, you know, it's justvery nebulous, andthose usually, you're kind of like, umm - it may not do as well.Okay, so here is our T stent.And we can kind of trim off a little bit more of this, and there's nomagic ratio or size or anything. It's just, we’re creating a little stent justto go in there. Let me have now some irrigation.And a damp sponge.Oh, jeez.Okay, a damp sponge.Go ahead and just try to get some of the ink off of it.Okay, now, Ariel - can I have a pair of smooth alligators and a Gimmick?So now we have to kind of get this situated how we're going to put it in.So we take it.Gimmick?And what we want to do is we want to fold these little T-armsover on themself -like so - one there,and then one like that, and then we grab itso that when we put it in, those little arms will kind of springopen - will you hold that like this? And then I need a -let me have that irrigation one more time.
Then I need that 5910 sickle knife,and then I'm going to need a - that thing is all bent.I'm going to need a...Okay, let's have the sickle knife - footplate hook.So now we are going to make just a little small incision right here.The lumen of the sac has kind of this glisteny appearance to it.Now the - the footplate hook.Oh, a smaller one.Is there one smaller than that?No. Huh?No, that's the smallest one. Are you sure?There should be one smaller than that, Ariel.That kind of glisteny tissue.Now the shunt.And it's weird, you can't probably see it well on there, but the insideof the sac - it has almost this weird, glisteny kind of -like a weird, glistening-like surface to it.And it’s all the sac.Right there.And see how it kind of tents it all up? Mm hmm.Let's have that footplate hook again.That’s exactly...What you want it to do, and that's it.
CHAPTER 5
[No Dialogue.]