
Laparoscopic Left Adrenalectomy
Main Text
Table of Contents
Primary hyperaldosteronism refers to the autonomous secretion of the hormone aldosterone from the adrenal gland, resulting in low renin levels. This usually occurs in individuals between the ages of 30 to 50 years old. The majority of these cases are caused either by a solitary, functioning adrenal adenoma or aldosteronoma (70%) or by idiopathic bilateral hyperplasia (30%). Other uncommon causes include adrenal carcinoma and familial hyperaldosteronism. Patients typically present with hypokalemia and long-standing hypertension that is difficult to control despite multi-drug therapy; nevertheless, further tests are required for diagnosis. An elevated plasma aldosterone level with a suppressed plasma renin level is strongly suggestive of the diagnosis. Once confirmed, further evaluation should be directed toward determining if the cause is a unilateral aldosteronoma or bilateral adrenal hyperplasia. This is done through imaging studies and adrenal vein sampling. Unilateral aldosteronoma is best managed by adrenalectomy, with the laparoscopic approach being the preferred method. Bilateral adrenal hyperplasia is often best treated medically, because only 20%–30% benefit from surgery. Here, we present the case of a 48-year-old woman who had long-standing hypertension and hypokalemia and was found to have hyperaldosteronism and low renin levels. A CT scan showed a small mass in the left adrenal gland, and adrenal vein sampling showed higher levels of aldosterone on the left side than on the right, confirming a unilateral aldosteronoma. Laparoscopic access was gained, the adrenal gland was exposed, dissected by controlling the periadrenal tissues with the harmonic scalpel, the adrenal vein was then ligated, and the adrenal gland was removed.
Primary aldosteronism, or Conn’s syndrome, was first described in 1956.1 It is a common cause of secondary hypertension, accounting for between 1% and 10% of all patients with hypertension. The pathophysiology involves hypersecretion of aldosterone, either by primary aldosterone-producing tumors or by hyperplasia of the zona glomerulosa of the adrenal gland.2
Primary hyperaldosteronism is diagnosed by measuring aldosterone, renin, and potassium levels. Typically, patients have high aldosterone levels, low renin levels, and low potassium levels. Following laboratory investigations, it is imperative to locate the source of the excess aldosterone. This is often achieved with imaging studies. Adrenal vein sampling is also generally performed to determine the side that is producing excess aldosterone, especially in cases where imaging may be inconclusive. Primary hyperaldosteronism that is caused by an adrenal gland tumor is treated with adrenalectomy. Virtually 100% of patients experience normalization of their hypokalemia following successful surgery. Fewer, though still the majority, experience at least some degree of lowering of their blood pressure.
The patient is a 48-year-old woman who has long-standing hypertension, for which she had been treated with several medications. She was also noted to have hypokalemia, and eventually was sent to an endocrinologist who did appropriate blood testing to biochemically confirm that she had hyperaldosteronism with suppressed renin levels. She was therefore diagnosed with aldosteronism.
The patient had a CT scan showing a small left sided adrenocortical adenoma. She then underwent adrenal vein sampling. This confirmed excess aldosterone secretion on the left side with a very high aldosterone/cortisol ratio compared to the right side (aldo/cortisol ratio of >3, left:right).
There are no particular physical signs or symptoms of primary aldosteronism; however, chronic hypertension often results in left ventricular hypertrophy. This may be heard on auscultation as an S4 sound. The examiner may also hear carotid bruits. On neurological exam, there may be muscular weakness (secondary to hypokalemia) and mental status changes associated with hypertensive encephalopathy.
A CT scan revealed a small nodule in the left adrenal gland (Figure 1). The right-sided adrenal appeared normal. This finding, combined with adrenal vein sampling, strongly suggested that the patient should have her left adrenal gland removed.
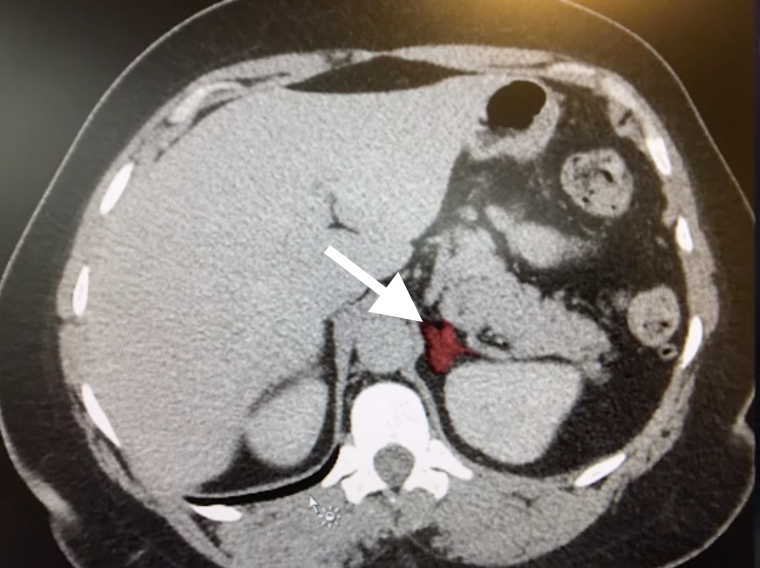
Figure 1. Abdominal CT Non-contrast CT image revealing a lesion (white arrow) in the area of the left adrenal gland.
Primary hyperaldosteronism is characterized by sequelae of hypokalemia and chronic hypertension. Muscle weakness, periodic paralysis and elevated serum creatine kinase levels secondary to hypokalemia have been reported prior to the detection of elevated blood pressure.3 Patients with long-standing hypertension are exposed to higher risks of major adverse cardiac events, including stroke, myocardial infarction, and atrial fibrillation.2
For patients with medication-resistant hypertension, a work-up for Conn’s syndrome is indicated. If a unilateral tumor is identified as the source of the excess aldosterone, surgery to remove the tumor is indicated. The options are most often laparoscopic or retroperitoneal procedures. These minimally invasive procedures rarely need to be converted to open procedures.
There are two reasons to remove these tumors: to correct the hypokalemia and to relieve the hypertension. The procedure reverses hypokalemia in virtually 100% of cases; however, patients are able to discontinue anti-hypertensive medications in only 35% of cases, this is likely because hypertension is often multifactorial (e.g., there may be an element of essential hypertension as well) or there may be occult disease on the contralateral side.4
Laparoscopic adrenalectomy is most effective when the disease is unilateral. Surgery is generally contraindicated in patients with bilateral disease; these patients are best treated medically with anti-hypertensives, espeically mineralocorticoid-blocking agents such as spironolactone.
Our patient underwent a successful resection of her left adrenal gland. The unusual features of the case included our finding of substantial amounts of adhesions in her abdomen without obvious cause. The tumor itself appeared hemorrhagic on gross examination. This is unusual in an aldosteronoma.
Most patients are able to go home either the same day or with a short < 24 hour hospital admission, provided they have no significant comorbidities. We decreased this patient’s blood pressure medications and had her monitor her blood pressure at home twice per day. We follow-up patients closely with telephone calls after the surgery and ensure that their blood pressure readings are monitored along with the serum potassium levels. We are confident that her potassium levels will normalize. It remains to be seen whether she will become normotensive, as she has other risk factors for hypertension, including obesity.
- Endo Catch Bag
Nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Conn JW, Louis LH. Primary aldosteronism, a new clinical entity. Annals of internal medicine. 1956 Jan 1;44(1):1-5.
- Cobb A, Aeddula NR. Primary Hyperaldosteronism. [Updated 2019 Apr 21]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539779/?report=classic.
- Olt S, Yaylaci S, Tatli L, Gunduz Y, Garip T, Tamer A. Hypokalemia-induced myopathy and massive creatine kinase elevation as first manifestation of Conn's syndrome. Niger Med J. 2013;54(4):283. doi: 10.4103/0300-1652.119658.
- Parthasarathy HK, Ménard J, White WB, et al. A double-blind, randomized study comparing the antihypertensive effect of eplerenone and spironolactone in patients with hypertension and evidence of primary aldosteronism. J Hypertens. 2011 May;29(5):980-90. doi:10.1097/HJH.0b013e3283455ca5.
Procedure Outline
Table of Contents
- Patient Procedure and Prep
- Procedure Outline Discussion
- Mark Trocar Position
- Insufflation
- Lysis of Adhesions
- Dissection and Removal of Adrenal Gland
- Transect Adrenal Vessels
- Extract Adrenal Gland
Transcription
CHAPTER 1
Hi. My name is Richard Hodin. I'm a surgeon at Massachusetts General Hospital and chief of our endocrine surgery unit. We're going to be doing a laparoscopic left adrenalectomy today for a patient with an aldosteronoma. This is a 48-year-old woman who has long-standing hypertension, has been on multiple medications, and was also noted to have hypokalemia, and eventually was sent to an endocrinologist who did the appropriate blood test and biochemically confirm that she had hyperaldosteronism with a suppressed renin level and was therefore diagnosed with aldosteronism.
And then she had a CAT scan. The CAT scan showed a normal right adrenal gland and a sort of the lobulated left adrenal gland with just a very small - what appeared to be an 8 millimeter nodule - not a huge mass but consistent with a small lesion that we often see with aldosteronomas. She went on to have adrenal vein sampling done, and this confirmed the step up on the left side with a very high all aldosterone level compared to the control cortisol, compared to the right side, so the ratio is quite high - over three - and therefore that confirmed that this was almost certainly a left-sided aldosteronoma. And we are going to remove the adrenal gland today, again, with a laparoscopic left adrenalectomy.
So this is the CAT scan, and it shows as we come down, a small adrenal nodule - not huge but clearly something abnormal in the adrenal gland. The right side of these images you can hardly see. It’s just a normal - a normal right sided adrenal. So with that imaging and confirmation with the adrenal vein sampling, we’re confident that this patient should have her left adrenal gland removed.
So the patient is being anesthetized now and Foley catheters being placed. I do a full lateral decubitus - almost 90 degrees, perhaps a little less like 80 degree tilt, and then we're going to use the transabdominal transperitoneal laparoscopic approach. I do a left paramedian open laparoscopic technique, so through the left paramedian position, we’ll place the Hasson trocar and then obtain a new perineum, and then we will place an 11 millimeter trocar in the epigastrium and two 5 millimeter trocars on the left costal margin or a little below that. And then we will mobilize things - mobilize the colon inferior medially - the spleen and tail of the pancreas to the patient's right and then circumferentially dissect the adrenal gland away from all of his attachments and find the adrenal vein which we will clip. And then the gland will be removed, placed into an Endo Catch bag, and bring it out. So that's the plan, and we’ll get started soon.
CHAPTER 2
Okay, we do a wide prep of the abdomen, chest, and back region just in case we have to make a open incision, and even theoretically, although I'm sure it won't happen, we will be able to do a thoracoabdominal incision. That's really not for this kind of case. I usually try to have the umbilicus visualized. We're going to go in a paramedian spot - so we’ll be above the umbilicus but just helps with visualization.
So here is the ribs, and what we're going to do is a paramedian, usually up a little bit superior to the umbilicus. If there's kind of - if there's a panis, I usually let it drop down and go a little bit lateral, and then there'll be some epigastric port. And then two 5 mm trocars out there. Can we have the local anesthesia?
CHAPTER 3
So I like to use preemptive analgesia which apparently works better than if you do it at the end. We do it at the end also, but I do it before. So we'll take the Bovie and sponge. So just use cut and make an incision there. Hold on one second. Let's make it a little bit longer going up. We’re gonna - okay. And then now coag. I'll take two Richardson's please. Okay so let’s go like this. You have a Schnidt please or a forceps? Use the corner. Okay so there - here hold this for me. Can I get a forceps please - the long DeBakeys? Oh - okay - just a Schnidt is fine.
So there's the anterior sheath. We’ll take a Bovie and just small incision, small. Up and down. Yep. Okay - stop. That’s enough. Okay, can we have zero vicryl please? So we’ll put stay stitches in. So go outside in, inside out. We’ll take a snap and scissors please. Grab that with a needle driver. Grab it with the needle grinder - the needle. I’m going to cut it. Okay snap, scissors please. You can cut it. Then another stitch. Let me do this again. Okay can you get the needle, see it? Cut that. Okay, snap. I'll take two S-retractors and another Schnidt please.
Okay so we have stay stitches in the anterior sheath. Hold on - you’re gonna - forget that - you can use this. On very thin patients of course, this is very easy. Okay take that out from it. Okay so I'm going to have you hold this one down here, if you want to grab - that's fine, okay - next to mine. Yep. Knife please. Can you hold that or not? Okay knife, and then we're going to take Hasson in just a minute. And I’ll just take this for a second. That's in there - yep. Hold like that. And like that - hold it like that. I just, once I get access especially - okay I'll take those out. Take it out. Alright. Is she relaxed? Hold like that. Okay. And then hold up the other stitch - trying to get a little bit of purchase. Okay - I’m going to secure this around here. You can put it up - it's okay up here.
We’ll take high flow on the CO2 please. And then, can we have the room lights off? And if you can put the pressure up - set it at 17 - 1. Looking in, we've got some adhesions - some sort of extra attachments of the omentum up here unfortunately. So we’ll have to take those down. We'll come in with our epigastric port. Okay so hold right here. Can I have the local anesthesia - yep. Okay knife please, and then the 11 mm trocar. Okay. Can I get the harmonic please? Let's start taking some of these down and we’ll get better access. I wonder if from the other side it wouldn't be easier though. Right here? Yeah I know, we'll do that but - it’s just I'm hitting her shoulder. I'm hitting the shoulder, but that's alright.
So she’s socked in here in the left upper quadrant for some reason - not sure why. Sure it has nothing to do with her - adrenal, but - not sure what. She hasn't had diverticulitis - let’s see yeah, obviously - or trauma - it’d be an unusual place for diverticulitis, but...
Okay, so what we are going to do now is put in the other two trocars - at least the lateral one first, so looking up towards the left upper quadrant. The colon - we obviously stay away from that - why don’t you bring it out there - horizontal or vertical? Horizontal 5 mm. And then… Good, and then why don't you to take this last adhesion down, and I'm going to take the fan retractor please. So let's take another - put another trocar in which will be about here, halfway between the paramedian and the latter one. Okay I'll take the fan retractor, just hold the scope for one minute please.
CHAPTER 4
So let's now continue by - that's fine - taking down the colon - the splenic flexure of the colon. We’ll just go zip right down and have the colon out of the way inferiorly and then we’ll... Let's take the scope out - wipe it first, and then put it in the - okay. Let's take these last attachments down up there. Down there. Let's get this stuff up here. Nikolai, can you open up every once in awhile to vent the port. Okay, hold on. Okay, go ahead. Okay so now, we don't really have to - we may want to drop it down a little bit more - just right there - just to give us a little more mobility, but then the key thing is next - is to get between the colon and the kidney.
Alright, so let's see, if you hold a scope for just a minute - sure thing. So, you see the colon there, right - and here's kidney that I'm sort of pressing on. So I open up this - let's get that later - before I go like this, you take your other instrument and just - take your other instrument and just push on the kidney back a little bit, so I push one direction - you push the other direction and that opens up the plane. So here down - look where I am down here - nope - no, that’s - you want to go - hold on one second. Right in there, and you push opposite me, and there's the plane right there. Go ahead. No, above. Above. Where you were - just right - get that stuff. Right there - yep. That's it. So it's an avascular plane between the kidney and the colon, and you go right in there, and you follow that. And that will lead us to where we’re gonna - and I come back and we still have to get the colon out a little more - see this? Go ahead - just get that. The harmonic is… Right there.
CHAPTER 5
So we're just getting again - push the kidney a little bit. Yep. There you go. That's the spot just the - yep. It’s all fizz fuzz. And then you come there, and you push the other direction, and it opens it right up. There you go. Get a little towards you more. Yep - and you’re a little too deep. Just get the fizz fuzz. I mean you should be right in here where my instrument is - you see it? You can almost see through it. Right there - yes. That's what you want. That's the spot. If you're in the right spot, it just completely unfolds. Go ahead and push. See it? Yep. Careful. You see what - what's undermeath - underneath me there? What is that, right there? So it’s either - pancreas? That’s pancreas. Yep.
So, now you can come up on top now. Get stuff up on top right there. And then you're going to follow this to get behind the spleen next. Keep going. See how we're going to head up, and that's how we're going to get the spleen mobilized. Go ahead - there we go. And you want to give yourself enough tension to see it, but not to tear anything - go ahead. Let's come down again - sure. Just push opposite right there - yep. There you go. And just follow that up. Nice. Okay, we’ll go in deeper. There we go - from the top, yep. And we’re going to carry this up all the way to the diaphragm - to the esophageal hiatus basically.
Okay and then we'll come back when you’ve sort of reached as far as you can go - you go again and then push opposite. So if you're in this correct plane - which you have to be - this tail of the pancreas is underneath my instrument, and then that exposes the adrenal gland, which is on your side. Do you see the adrenal gland yet? No - a little bit maybe. Okay, go ahead. I see it - you see it? Yes. Well, I’m glad. Right underneath there. Is this it? Yep. Okay. Alright, go ahead - go ahead, get that. What’s that? Leave that - that's - yeah, that’s on my side. You don't want that - you want to be on your side. Yep. Can go on there. Yep. Yep. Okay. Keep going there.
Is there an NG tube in? Or OG tube? Can you suck on it please? So as you come around the top, you just want to be careful of the - and the stomach which can - poke its head in. Yep. So just stay closer to the diaphragm a little bit - yeah, what you can see. So you - yeah, cuz the stomach's going to be underneath my retractor, and you just don't want to possibly hit it. And now I'm sort of retracting not only to the patient, you know, to the patient's right, but also kind of inferiorly bringing it off the diaphragm - how it comes down - see how it comes down. There's always little bit of fluid up here.
And then - now we'll keep going where's your other instrument - just okay - that's fine, yep, so let's go up here and just finish that. So you see the stomach there? That's why we have to be careful. And it's gonna - but I'm sort of trying to protect it with this fan and then - yeah, just get that single layer going up all the way. Yep, just let everything drop down in terms of the stomach, and okay, so now let's come back this way.
Let's look again - we’re going to get better exposure so the adrenal gland is right under there. You can see it. It's covered by normal layer. Okay so now go opposite of me with your other instrument - where are you? Just go right in there and just push a little bit on your side and then you'll open up that plane and keep going, yep - hold on. Let’s make sure we're here - you should be up. Go a little closer, closer up there. So right, yeah - right - right in that's fine. Just get that a little bit, yep, well. There was a plane there, see it there? There we go.
Now this is all now getting - see how it’s going - now the key blood vessel I always look for is the phrenic. The phrenic comes down off the diaphragm and runs down here, and the adrenal gland which is touching right there - that's the edge of it, you can almost see the edge - and then right under there running this way is going to be the phrenic. And what you want to do is be right between the adrenal and the phrenic.
So I'm actually going to ask you to take this - hold on one second. Let's do this - little bit more first, and then go this way. Then I'm going to show you cuz it's a little difficult to explain. Let’s get a little more exposure here. Go ahead. Push a little opposite maybe - just kind of the adrenal. Yep. There you go. Towards you a little more. Okay.
Okay so what I'm going to ask you to do is come over here. Okay, so you're going to go in with the - look in with the scope, and you're going to go this way - just carefully cuz you have the spleen and the pancreas, right? Here is the edge of adrenal. Right - so I'm going to go like this and just kind of - see the edge? Look look right in there where my instrument is. You can - no, right there, yeah. So we - so you want to sort of hug that because there's not much tissue there, but that's going to keep you right on the - the correct side of the phrenic vessel. And once you go like that, and I take my other instrument and pull it over, and now we're going to head north, superiorly, and just detach it from the retroperitoneal attachments in the diaphragm.
Now depending if it's cancer you’re operating on, you may do a wider resection in terms of the periadrenal fat - doesn't hurt to take the periadrenal fat, but you don't have to for something like a benign aldosteronoma, which is this case. So it comes right off the muscle. This plane is almost always - essentially always - sort of intact unless somebody's had prior surgery or some unusual. So I just make my way through this fat, and I'm pulling with the other instrument kind of down, so that I know I have the adrenal gland on sort of my side.
Okay, I'll come this way, so let's now look again where we were here over - look over here. So now here's the edge of adrenal, so - but if you follow the phrenic, you’ll always get to it. Look over - look right in here. So we're going to stay along this line. Now I usually mobilize the entire adrenal or most of the adrenal before getting the vein but sometimes - depends on the case. And if you have a pheochromocytoma specially if there's any kind of hypertension with manipulation.
Can I get the suction irrigation? So I often will use a section irrigator - can you clean that for me please? How's my other instrument? That way I can keep it dry of blood and fluid. Let's see - pull back or - can you straighten out the scope please? Now your instrument - where's your fan? You can come closer to me.
Here’s the renal vein which you can see very - and here's the adrenal vein. You can always get around the adrenal vein very easily - almost always. I just want to clean this up and then - okay. So there - we’re underneath the adrenal, right? And then here is the vein, which we can get any time, but I just want to show here - now coming this way. So a lot of times, I’ll dissect out laterally first, so look over here - here's kidney, and you look for the cleft between the - between the adrenal and the kidney. You have to and then - you have to incise here, and you want to find the natural cleft between kidney and adrenal. There is adrenal gland there. So here is - the adrenal’s over on that side and the kidney’s here, so you just once you find that spot you can just go zip zip. Take it right out - see the kidney’s right there, so you hugged the kidney right there. Once you find it - it's - you can just easily take this off. And again depending upon the pathology, you can go out and take more of the periadrenal and even perinephric fat. But here is again a vascular plane right on the kidney, so it's easy to take this, and then we're going to get it down to the muscle so we meet where the dissection was above.
So again we're just getting the periadrenal fat, and it's going to come - we - we did a lot of work from above or the other side, so it's - it becomes very easy to go here and we - get the - sort of connect-the-dots. Should I bring my fan over? Let's look down here - I don’t have much left, right? Because here's the adrenal - yep. Now sometimes this bit here is a little bit more difficult, but in this case it's not that difficult but you want to get superficially - to follow the adrenal - sometimes there's a tongue that goes down inferiorly more towards the kidney, and you have to kind of make sure. Do a little bit of the dissection there just to make sure that we're below kidney kick - I'm sorry, the capsule of the adrenal - but I feel pretty confident now that we are, so it's basically going to be all done except the vein. Do we have that 5 mm clip applier? The patient doing okay?
So we have the adrenal on its pedicle - pretty simple huh? And then we'll just go like this - no, I'm sorry - I'll take the clip applier. So you load, and then you put it in. Hi Heather. Alright, let’s do the scissors, and then we’ll take a bile grasper please. Harmonic. Let’s take that bile grasper please, so I’ll grasp it- not where the actual adrenal is or the tumor. Okay we're going to go like that, and can we have some Trendelenburg and a shift to the patient's left? So we'll just irrigate a little bit - everything looks - so there's our clip. Little more Trendelenburg and shift to the left please. Let’s just look at the - come back with the scope now and look - look at the spleen and pancreas kind of - yep, that's fine. Let's put the scope in there. We’ll take an endocatch bag please.
So can you - yeah, you’re straight - right? Where is the - find the adrenal - right there. Yeah, that can you come out. Okay. Drop it in. Nice. That's good - take that please. Okay so looks good, right? So let's look at these trocars and we pull - take them out. Those sites look fine. Okay and that can come out, and room lights on please.
We can have the Kelly please. Came out easily cuz it’s small. Scissors. So we'll take a look at this in a minute, so don't put that anywhere. Okay can I have a wet sponge please? Left adrenal. And 2 narrow Richardson's and the Bonnies and 0 vicryl. So I usually do stitch above, stitch below and then tie the ones together that - that does it - in cases where - it’s slightly larger.
CHAPTER 6
Yeah, if we have to enlarge it to take the adrenal gland out, then I’ll often just run this layer. And I’ll just do a figure of 8 just to... Yep great. Okay, then let's tie those together real well. Tie them like across from here? Yeah, yeah, just like that. And I'll take the wet sponge. Okay, more local anesthesia please.
And then post-op for this lady, she gets - she's going to go home if she's okay. I've been sending - Home? Yeah. Depends of course on the underlying disease. Pheochromocytomas, those patients don't go home. Obviously, if somebody has medical comorbidities, they don’t go home, but for - I'll take some more - for cases like this, if they feel up to it, it's fine. The incisions are basically the same as for a lap coly, so it's different on the inside, but on the outside it's pretty much the same and the recovery shouldn't be that much different. Now, theoretically, with aldosteronomas of course, they have a high blood pressure, and if their blood pressure is a problem at all in the recovery room or early post-op, then we would keep them for observation.
So this patient, like a lot of patients with aldosteronomas, you don't know for sure - what - you know, how much their hypertension is going to respond to the surgery. If you fix the aldosterone problem, which I’m sure we did, then her hypokalemia will resolve that problem, and very likely her - high blood pressure will be a lot better - easier to control and possibly even go away completely, but on the other hand she has other risk factors for hypertension. And this may not make her normal tensive. That'll be something we’ll have to figure out over time. I generally have patients take their blood pressure at home couple times a day, write it down, so that we can have access to that information. The primary care doc can have access to the information. She also has an endocrinologist who she's been working with in terms of blood pressure control so.
So I'm going to want to look at the specimen.
CHAPTER 7
I'll take a knife please. Yeah, that blade. You can see - I can - I think see where the tumor is, but we'll see. I'm just bisecting a gland. So this is - there's actually been some hemorrhage inside this lesion which is right here. So that's a little bit unusual for aldosteronoma - not sure what to make of that - but you can see the lesion here. And then more normal adrenal. Adrenal. That's more normal-looking adrenal tissue with the cortex of the yellow on the outside and the brown medulla. Put the light on it for a second - I’ll show you.
So this is the normal adjacent adrenal’s cortex has a yellow color and then the medulla in the middle - brown - that's normal adrenal. This is the lesion which you can see there's you know it’s the rounded lesion, but there’s hemorrhage in the middle. Interesting. That doesn't happen so often without astronomos compared to some other kind of lesions, but not sure - we’ll wait for the final pathology I assume it’s just a benign adenoma. Yeah. So we've finished the closure just putting steri-strips and little dressings on and then she’ll wake up and go to the recovery room for a couple hours, and we'll keep an eye on her for at least 3 or 4 hours today. And if she's okay, she can go home.
CHAPTER 8
So we’ve finished up with the laparoscopic left adrenalectomy. The patient’s being woken from anesthesia. Everything went well with the surgery. The only surprise you find was in the beginning with all the adhesions from the splenic flexure of the colon up to the abdominal wall. You always see some attachments, but this was much more unusual, and I'm not sure if there's been previous inflammation in that area. We didn't see anything abnormal other than that, but in any case, once we took those down, everything else was pretty straightforward and found that tumor in the adrenal, which we opened up by at the end, which did have some hemorrhage in the middle, which I think is a little unusual for aldosteronomas but not really too concerned about anything like a malignancy in this case.
And the expectation is that the patient will have her hypokalemia fixed. The blood pressure response over time - we’ll have to see how much of her hypertension responds to the operation. I'm hoping that she can go home today - a lot of these patients can - but we'll see how she does in the recovery room and for a couple hours afterwards. And - and she’ll - in any case, monitor her blood pressure at home, and I will keep in touch with her closely to make sure that she's on the right medications over the next couple weeks as she recovers from the surgery.