
Arthroscopic Total Shoulder Resurfacing with Osteochondral Allograft
, University Hospitals of Cleveland, Case Medical Center
Main Text
Table of Contents
Limited treatment options exist for glenohumeral osteoarthritis in a young and active patient. To address the pain and limitation of significant osteoarthritis while avoiding a total shoulder arthroplasty (TSA), we have been using a minimally invasive technique to resurface both the glenoid and the humeral head using osteochondral allografts. After identifying the areas of most severe chondral damage during a diagnostic arthroscopy, a transhumeral tunnel is drilled using a transhumeral guidepin. Through this tunnel the allograft donor sites are prepared by retrograde reaming the humeral head and antegrade reaming the glenoid socket. Allograft constructs are sized and cut intra-operatively on a back table, inserted through the anterior portal and secured into the graft sites using chondral darts for the glenoid and a press fit for the humeral head.
This is a 53 year old right hand dominant male with right shoulder pain gradually worsening over the past three years. His pain is worse at night and with overhead motions and rates his pain as a 7-8 out of 10 at its worst. He has slightly decreased range of motion, most notably in internal rotation, and pain upon overhead lifting and forward flexion above 140 degrees. His pain interferes with his work as well as his quality of life, interfering with restful sleep.
He reports no loss of strength or numbness. Past history is significant for Type 2 Diabetes Mellitus and hypertension. He has had 2 corticosteroid injections which resulted in minimal pain relief. Treatment options were discussed with the patient, including observation, activity modification, repeat injections, occupational therapy and total shoulder replacement versus arthroscopic surgery to resurface the shoulder with allograft. Risks and benefits were discussed in detail with the patient and he requested the arthroscopic resurfacing procedure.
On exam, he reported a pain severity of 7 out of 10 on forward flexion above 120 degrees. The shoulder is stable with a negative lift off test and there was no weakness appreciated to the rotator cuff upon static strength testing. There is mild loss of motion in all planes, with forward elevation to 160 degrees, external rotation to 40 degrees and internal rotation to L5. Passive range of motion is comparable to active range of motion with stiff end points in all planes. He has positive impingement signs, a positive speeds test and tenderness to palpation over the anterior aspect of his shoulder in the region of the proximal biceps tendon. He is neurovascularly intact distally to his right upper extremity with full range of motion to his right elbow, wrist and hand.
Pre-operative AP and axillary radiographs reveal severe narrowing of the glenohumeral joint space and subchondral sclerosis
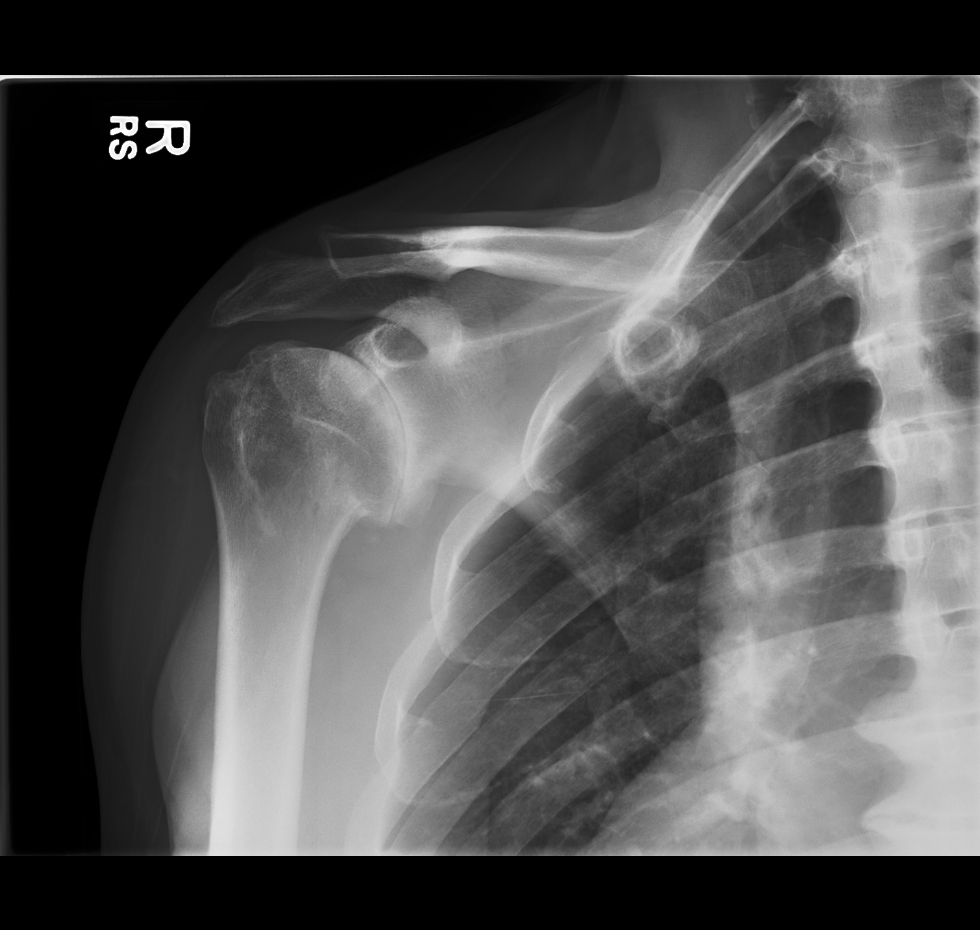 Anterior-Posterior View
Anterior-Posterior View Axillary view
Axillary viewWithout intervention the expected natural clinical progression consists of worsening pain, increased severity of osteoarthritis, and further decreased shoulder range of motion.
The options for treatment at this time include a repeat corticosteroid injection, physical therapy, NSAIDs, a total shoulder replacement, arthroscopic debridement and a resurfacing procedure with allograft.
This procedure avoids a total shoulder replacement in a relatively younger and active patient. Advantages include a shortened recovery period, no loss of strength, the subscapularis is kept intact and the relatively high risk of TSA implant failure in younger patients is avoided. As opposed to an open procedure, arthroscopy is less traumatic, has less risk of joint infection and allows for complete visualization of the shoulder joint.
The larger size of this patient's shoulder makes for a slightly challenging case. If the osteoarthritis was more extensive, the patient was not particularly active and over the age of 60 years, a total shoulder replacement would have been recommended.
Care needs to be taken when placing the transhumeral guide pin; the axillary nerve should be identified and kept clear of pin placement by blunt dissection down to the humeral cortex.
In a larger shoulder such as in this case, it is especially important to take care when inserting the allograft through the anterior arthroscopic portal not to lose control of the graft as retrieval would be potentially difficult.
Glenohumeral arthritis remains a challenging issue to treat in the active young patient. This is due in most part to concerns regarding the longevity of a stable total shoulder prosthesis, specifically loosening, failure, and the eventual need for revision surgery. Young patients that wish to maintain a high level of activity may not be suited for traditional total shoulder replacement because of this concern of implant durability. Arthroscopic biologic total shoulder resurfacing with osteochondral allograft can be a promising alternative for the treatment of arthritis in a young individual. It also allows for bone conservation, so should the arthritis progress, a standard total shoulder replacement can readily be performed at a later date, if necessary.
This procedure has been performed by the senior author (RG) on 22 patients with a 2 year follow-up. Results have been promising with improvements in mean visual analog pain scores improving from 6 to 1. Range of motion in forward elevation has improved on average from 128 degrees to 137 degrees. The mean American Shoulder and Elbow Surgeons score in this patient population has also improved from 40 to 83. However, long term outcomes are not yet available.
Disclosures R.G is a consultant for and receives support from Arthrex, Naples FL
Informed consent was obtained from the patient and all staff present in the operating room to be filmed and are aware that portions of this video will be published and freely available online.
- Arthroscope - Stryker, Kalamazoo MI
- Chondral Dart System - Arthrex, Naples FL
- OATS system - Arthrex, Naples, FL
The authors would like to thank Ian Fein for his videography and the Operating Room staff for their help in making this video.
Citations
- Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS. Total shoulder arthroplasty versus hemiarthroplasty: indications for glenoid resurfacing. J Arthroplasty. 1990;5(4):329-336. doi:10.1016/S0883-5403(08)80092-7.
- Wallace AL, Phillips RL, MacDougal GA, Walsh WR, Sonnabend DH. Resurfacing of the glenoid in total shoulder arthroplasty. A comparison, at a mean of five years, of prostheses inserted with and without cement. J Bone Joint Surg Am. 1999;81(4):510-518. doi:10.2106/00004623-199904000-00008.
- Burkhead WZ Jr, Hutton KS. Biologic resurfacing of the glenoid with hemiarthroplasty of the shoulder. J Shoulder Elbow Surg. 1995;4(4):263-270. doi:10.1016/S1058-2746(05)80019-9.
- Gobezie R, Lenarz CJ, Wanner JP, Streit JJ. All-arthroscopic biologic total shoulder resurfacing. Arthroscopy. 2011;27(11):1588-1593. doi:10.1016/j.arthro.2011.07.008.
- Millett PJ, Gobezie R, Boykin RE. Shoulder osteoarthritis: diagnosis and management. Am Fam Physician. 2008;78(5):605-611. https://www.aafp.org/afp/2008/0901/p605.html.
- Dubrow S, Gobezie R. Alternative options to traditional shoulder replacement: arthritis in the young patient. Curr Orthop Pract. 2013;24(4):370-375. doi:10.1097/BCO.0b013e318296b065.
- Dubrow S, Shishani Y, Gobezie R. Arthroscopic alternatives to total shoulder arthroplasty: you have got to be kidding. Semin Arthroplasty. 2013;24(1):2-6. doi:10.1053/j.sart.2013.04.003.
Cite this article
Ruben Gobezie, MD, Samuel Dubrow, MD. Arthroscopic total shoulder resurfacing with osteochondral allograft. J Med Insight. 2014;2014(1). https://doi.org/10.24296/jomi/1Procedure Outline
Table of Contents
- An Interscalene block was placed in the preoperative holding area.
- Place patient supine on a Tenet beach chair with a Spider arm holder.
- Prep and drape the upper extremity in standard fashion for this procedure.
- Introduce an arthroscope in the standard posterior portal into the glenohumeral joint. Make a standard anterior portal through the rotator interval using an 18-gauge spinal needle for guidance.
- Perform a systematic diagnostic arthroscopy
- Findings: On inspection of glenohumeral joint, there was severe grade 4 arthritis in both the humeral head and glenoid. There was an intact superior rotator cuff. There was superior labral tearing with type I vs type II tears visualized. There was a tight shoulder capsule and extensive synovitis within the glenohumeral joint
- Perform arthroscopic biceps tenotomy with an Arthrocare ablator device at the insertion of the biceps onto the glenoid labrum. Using the anterior portal, the biceps was observed to retract within the groove.
- Open-subpectoral biceps tenodesis
- Make an axillary incision as is standard for this procedure.
- Incise to pectoralis major fascia.
- Place a pointed Hohmann retractor underneath the pectoralis major over the lateral humerus.
- Place a finger retractor medially.
- Identify the biceps sheath and open it.
- Pull the biceps stump from the shoulder and whip-stitch it with Arthrex fiber loop #2 fiberwire.
- Cut the needle off and put the sutures through the biceps button.
- Drill a 2.7 mm drill hole bicortically and ream the anterior cortex with a 7mm reamer.
- Insert the button into the drilled hole and "flip" on the posterior cortex.
- Tie the suture to secure the tenodesis.
- Continue the arthroscopy.
- Resect the entire rotator interval
- While viewing from the posterior portal, insert the humeral head guide through the anterior portal. This will center the transhumeral guide pin onto the humeral head lesion.
- Make a skin incision on the deltoid where guide pin contacts the lateral deltoid. Dissect down to the humerus with a Schnitt to make sure there is no axillary nerve encroachment
- Drill an Acorn guide checking the position through the anterior and posterior portals.
- In this case: A 4.5 mm guide was used. Knock pin in until an assistant can grasp it through the anterior portal
- A 5.5mm cannulated drill is then advanced over the guide pin and into the subchondral bone of the humeral head
- A transhumeral sleeve is placed over the portal dilator until visualized in the glenohumeral joint.
- Insert a 20 mm retrograde reamer (Arthrex) through the anterior portal, assemble reamer/drill apparatus within the joint
- Pull the transhumeral sleeve back out 5mm
- Retrograde ream the humeral head to a 20 mm depth by running the reamer on forward and pulling the reamer laterally, pressing it against the humeral head articular surface.
- Disengage the reamer bit from shaft pin using T-handle.
- Manipulate arm until transhumeral sleeve is centered over glenoid bare spot.
- Drill the self-tapping drill bit into the glenoid bare spot.
- Disassemble the guide apparatus
- Insert the antegrade reamer and attach shaft pin to reamer, manipulating arm as needed to allow attachment
- Once attached, manipulate reamer until centered in the nipple created by self-tapping drill bit
- Ream to 20 mm until completely flat on all surfaces.
- Move camera to anterior portal to inspect reaming. Continue to ream.
- Disengage the antegrade reamer from the shaft pin.
- Reinsert the 30 mm humeral retrograde reamer and retrograde ream to 30 mm humeral flap.
- Disengage reamer from the shaft pin.
- In this case: The proximal humerus graft was fashioned by using a series of sizing guides as described in my paper in the Journal of Arthroscopy (ref. 4). In this case we used a humeral graft with a diameter of 30 mm and a width of 5mm.
- Using a distal tibia I did the same for the glenoid graft to fashion a graft with a diameter of 20 mm and width of 5 mm.
- A drill hole is made through the center of the humeral graft and a suture is placed through in order to help position the graft into the humeral head defect. The suture will later be used to pull the humeral graft into proper position on the humeral head, through the transhumeral guide.
- Insert the glenoid graft (in this case, taken from a distal tibial plafond) into the glenohumeral joint. Impact the graft into the glenoid position using the Chondral Dart System (Arthrex, Naples FL) using the Chondral Dart drill guide to hold the graft into position.
- Position the graft into defect.
- Place 3 chondral darts on the glenoid. Get a good fixation and press fit.
- Place the Nitinol wire loop through the chondral dart apparatus and retrieve through the anterior portal.
- Use Nitinol wire loop to grasp the suture previously placed on back table through the 30 mm graft
- Place humeral graft through anterior portal.
- Retrieve Nitinol wire loop grasping the suture and manipulate with a finger through the anterior portal until graft is well seated into the glenoid defect.
- Ensure a good press-fit fixation.
- Close all the portals after removal of all instruments from the shoulder with buried interrupted 4-0 Maxon sutures. Place the patient in a sling.
Due to the fact that this is an arthroscopic technique that leaves the subscapularis tendon undisturbed, rehabilitation can occur quicker than in a standard total shoulder replacement. The patient was kept in a sling for 1 week with passive range of motion starting the first week post-operatively. Full active range of motion was initiated at 2 weeks post-operatively and strengthening was started at 6 weeks. At 3 months out he achieved active range of motion as follows: forward elevation to 170 degrees, external rotation to 50 degrees, internal rotation to the L1 vertebral level. The patient had excellent pain relief, with no loss of strength or paresthesias. AP and axillary x-rays demonstrated well seated grafts with a smooth articular surface and increased joint space.
 Anterior-Posterior ViewAxillary view
Anterior-Posterior ViewAxillary viewTranscription
INTRODUCTION
So my name is Reuben Gobezie. I'm the chief of the shoulder and elbow service at University Hospitals of Cleveland, Case Medical Center. And what we're going to do today is we’re going to review a new or relatively new procedure called arthroscopic biological total shoulder resurfacing. So this is an arthroscopic surgery, and essentially what we do in order to achieve a cartilage transplant in the shoulder using this technique is - we bring the patient in. You'll see when we first put the scope in the shoulder, I'll do a routine diagnostic arthroscopy, look at everything, make sure the rotator cuff is intact, make sure that - that the chondral loss is what I thought it was going to be before the surgery, and then size up the humeral head and the glenoid graft sizes cuz there are different sizes I can transplant. Next we're gonna - you're going to see that we take out the rotator interval and remove the biceps from the field - gives us more working room - and then we'll start with the procedure where we start to reprepare the surfaces of the humeral head and the glenoid so that they can receive the graft.
This is a - a patient that essentially has classic osteoarthritis of the shoulder, albeit at a young age, and the options for him today in my practice would be a total shoulder placement with conventional prostheses or one of these alternative graft procedures not osteochondral graft, which I think don’t - have - have fallen out of favor - I don’t use it anymore - or this osteochondral grafting. I think - debridement has already been tried; it did not work for him and so here’s where we’re at - basically a bipolar graft.
CHAPTER 1
Okay good. So here we have the glenohumeral joint, and you see here is that there is a - some grade one and two and three changes. Then you get down to here, and you see there's a grade four change. See what I mean? There’s a grade 4 change. Likewise on the humerus, it’s completely denuded of cartilage. It’s a grade 4. So you get way up here, and you can see that there is some cartilage there. The rotator interval is here. The subscap is there. And then the vy - the rotator cuff superiorly is still intact, right there. And then he has, of course, a normal degenerative superior fraying, te - tenotomized the biceps already. And now what we’re going to do is we’re going to go into the rest of the surgery here.
CHAPTER 2
We’re going to resect the rotator interval now. And essentially that’s what we’re going to do now; we’re going to resect the rotator interval. These are very, you know, every - each - each of these arthroscopic totals are done in a very different character and - and based on the soft tissue tightness of the shoulder and so on. So here I’m going all the way out with the rotator interval resection. You have to go all the way out past - just the capsule that’s deep - and all the way out until you see deltoid fibers because, when you’re passing instrumentation, you really want to be careful to make sure that you get that so you can pass instruments easily, you see? And then you can see here, the conjoined tendon is coming up in the left side of your screen there, here. And then what we're going to do is widen the skin incision, and then we’re going to put a drill guide here, which is 25 mm in diameter. And visualization is key because you have such m - so much outflow. I'm introducing now the - the guide, and you see here that I keep this guide - you have to be very careful of the axillary nerve here, and I keep this guide here in a position where I feel like I can assess the humeral head. And there you go.
Okay I think that's a good position for it. I'm going to go below the center cuz, remember, it’s only a 35 mm guide. I’m going to go below the center here where... Okay good - and hold that, Sam, for me. Now I'm going to come out, and I’m going to take this and I'm going to do this, here. Okay, knife. Eleven-blade, Gaby. Eleven-blade. Okay, good. And that tells me where it is in the skin. It’s kind of the angle. Show me the - show me it sitting on the b - bone. There you go, good. And then I’m going to make an incision here. Okay and then what I’m going to do next is I’m going to spread with the - a schnidt because the axillary nerve is here, and I can tell you, I had a scare recently where I had a - a - not a palsy - yeah, I had a transient palsy. Let me tell you something, it’s a - a game changer - makes this procedure not worth it if you can’t obviously get - if you get a nerve palsy.
Okay good, and then so now what I’m going to do is I'm going to slide this little groove in there and then - feed that for me, feed that - there you go. See the pin’s there. So remove this - take a mallet - and then what you do - and then a grasper for the pin, and what I do is knock it in so my assistant can hold it. So here we go. So, you just grab this here. And okay, so this one still has a loop on it. It’s the old one, but it should be fine. Okay. So then you grab it like that. So now we want a dilator, tissue protector there and next. Okay good. Alright, so here’ a 55 - 5.5 millimeter reamer and... oh. Take off the tissue protector and you go to the 5-5 reamer, and then basically it’s going to go through the outer cortex of the humerus.
Okay. Okay guys. I’m going to take this out. This needs to come off first. Okay good. Alright, good. So now we’re going to go in and put the transhumeral sleeve there. Good, now you can let go. Now we can take it off. Okay good. So now what you have here is a… the transhumeral sleeve, and you see here - can you stop the outflow? You see here that that’s really in the center of the head.
CHAPTER 3
Now what we’re going to do is go progressively to the reamers. So - yes, thanks. You’re going to take a 20 millimeter reamer, okay and you’re going to introduce that into the shoulder joint first. Just introduce that right into the shoulder joint through the rotator interval that you see there. And then what we’ll do is - sometimes I put a little bit of pressure on the arm to get it open like that. And then I’ll take the stick, the transhumeral sleeve, guide, and pin, and I’ll put that in there like that. And now I just need to see where is that central bit there, and it’s right down there. Just kind of have to work it in there. And once you get that in there, boom! Just lock it in there like that. Usually, it goes in without too much difficulty. And you see that that’s locked in there. And then you’re ready to retrograde ream.
So now, we’re going to take the drill - okay, good. And then what we’re going to do is pull back on the sleeve here. It locks on, and then we’re ready to go. And hopefully it doesn’t take us too long. I’ll pull back on the - on the transhumeral sleeve here - try to get some better tissue. And you just gotta apply gentle traction and be very patient.
So now what I’ll do is I’ll go into the anterior portal here. Back up. T handle on this thing for me. T handle. And then I’ll put the T handle on here. Yep. And I’ll back this - just unwind this thing here. It’s kind of cool because you’re putting the instruments together in vivo - you know, inside the shoulder joint. And what you see here - then yea, exactly. See I’m showing you? What you see here now is a nicely appointed humeral head resurfacing. I don’t think we’re going to have to go much bigger than that on the joint - on the humer. I think it looks pretty good. Now the glenoid - because that’s really where the action is on this guy’s shoulder.
CHAPTER 4
Okay so now, again, I’m going to center this where I think the biggest part of the pathology is, and I just position the arm in a way that I feel like it will help me achieve that goal. So you see here that the arthritis is down there, and you kind of want this glenoid resurfacing to be where the arthritis is. So now the question is getting the arm in the right position for the transhumeral sleeve. Is always fun. To me - okay, good. Okay. Okay good. And then turn your eyes the other way so I can see the glenoid and make sure that I’m in the right spot with the glenoid. Make that - we’re just going to bury this to the harvest and back out. Okay. And then what we’ll do is take this down here. You can sort of back this out a little bit. Show me what’s going on here please. Back this out a little bit here, so you can disconnect those two. And then you can pull this out. Okay cool. So then, again, I’m going to introduce those anagrade reamer now, and that’s going to beone where I kinda have to see where I'm coming in from. The anagrade reamer - looks like I lost it. Somehow I need to…
Let' see here. Alright, so now - now what I’m going to do is find out where’s that nipple. Keep your hand there just cuz I - I need to just kind of think - okay, good. I’m going to try and find that nipple here. Okay, so that nipple needs to be buried in there. What I’m going to do to do that is, sometimes I move the arm in the armpit, a little bit out. You know what I mean? there you go. It seems to fit right in there. So, you see what I’m doing? So this is technically a demanding operation for this reason. Really, it requires every skill you have in arthroscopy: anterior portal visualization, posterior portal visualization, orientation - I mean literally - it’s like everything. So, you know. Okay so now we’ve got to get this thing back into this hole. Once you get in there, it’s kind of refreshing and nice and all that good stuff. Okay and then use that to manipulate it, and there you go. Once you get in - okay, right there - that’s it. Okay good. Okay is this a drill?
Okay so now I’ll basically - I’ll basically just ream it. And this is the hardest - usually, the hardest part of the reaming job. Yeah, okay good - we’re getting what we want out of this thing, you see that? Just - you just have to double check and make sure that you’re getting what you need out of this thing. And sometimes, what I’ll do is I’ll move it to the anterior portal for this portion, and for whatever reason, it seems that this is a good position to see my - yeah, can you hold that? Thank you. Forgot about that. It’s a good portion - position to see my reaming. Yeah it is, right there - okay good. So there’s - there’s the view I’m looking for there. Put that in. Okay good. Give me that view there. And so, now what I do usually is I - I stick this - no - this way. Got to - I start to - to move the shoulder so that I can close the goal - hole, if you will. Yea, that gap right there. I think we got a good rim there, good rim there, good rim there, good rim there. I think it looks good.
Okay, so now what we’re going to do is prep the humeral head cuz that’s done already on that side too. Alright, and then… Yeah.
CHAPTER 5
What we really want to do is the K wires. View your side - your side. You can put it back in that holster. Hammer or drill? Huh, that's kind of misleading, huh? Why is that moving? It’s pretty cool, isn’t it? Okay, so now what we get to do is saw the top off. So what we really need are some good holdings on this thing. Yeah, I’m going to need you to do it in a way that you - I can still get in there. Yeah. Don't let that thing come out - come out of there. Okay. So there it is, there. By 5 millimeters, right? Five millimeters good?
Here’s a tibial - here’s a distal tibia. This is an ankle joint. And then we’re going to put this similarly. Okay good. So now we take that out like this. You want to hold? So once again we got a nice little graft - but you see how it’s U-ed there? It’s never going to be flat when you put it in a scope. So just remember that it doesn’t matter. Twenty - that’s fine. Twenty millimeter by five millimeter depth. And so this one… Here it is - a 20-by-5 millimeter and that - that’s quite thin, which is typical of a distal tibia. Okay, let’s have the - let’s have the pulsed lavage. Let’s have a fresh bowl and a pulsed lavage. Alright - just to clean off the person’s - you know - own blood. Okay. Cool. Okay. And a knife back to you. Now we’re going to do this, and we’re going to - this is from the blood - patient’s own blood. It’s called ACP, you know what I mean? And basically, it’s - it’s a platelet-rich plasma der - basically derivative version of that. Okay, so let’s get back into the shoulders, let’s get back to the real part of the surgery here.
CHAPTER 6
Grafting place is right here. There’s the graft side. And it’s sort of finicky, but it’s pretty cool. Okay so now, what we’re going to do is we’re going to insert the graft. Very important step here: not to lose the cannulation. I think that’s where I got that exterior nerve last time. So don’t let me pull that out, okay? Here, hold it up here. Hold it up there. Hold that. Hold that. Don’t let go right now. I need - I need you to help me because I can’t - this is where it gets kind of tricky. Pretty much in the site isn’t it? Okay. Isn’t it pretty much in site? Looks like to me too. Yeah it’s in there. It’s in the site there, so - see there? Good. Almost seems like a…
Okay, implant. Plunger. Shoot. That drill - that - that - that bone is really good. Okay, so that’s okay. What we’ll do is we’ll come back and get that guy in a second. Okay so now let’s go and do round two. Okay good, drill. Help me. Kind of go in-and-out to really get that thing in there. That went in a lot there. You should grab - you saw that disc? Guess we just get rid of this. There you go.
CHAPTER 7
Grasper. Okay. Okay let go. Just come in with this grasper here. Okay, good. Good. Good. Okay. Good. Right in his right. Ohhhhhh. Ahhhhhhh. Really good. Okay good. No, no just ta - Okay guys, thanks everybody.
I think it’s a well recognized need in our field - that is to say, trying to address successfully the arthritis in a young patient. And we know from the literature, the group - work done out of Mayo Clinic and others - where essentially, young patients, who have a shoulder arthroplasty, they don’t last as long, and their satisfaction is less. And trying to address that issue. And there have been many different ways people have done it through biologically grafting, using Achilles tendons, dermal matrices, and so on. Not satisfactory results, so the natural next, in my mind, move was to go where the knee had gone several decades ago and - and - and really try to develop this area of cartilage transplant for the shoulder. And it's nice because osteochondral graft is really the only way, to this day, that we have of making a graft or chondral procedure that is biomimetic - that actually reproduces the mature, hyaline cadage - cartilage that you’d see in a - in a normal joint. The rest of them really don’t reproduce that. You know, the - the microfractures, the autologous chondrocyte implantations - they don’t - they don’t achieve that whereas the chondrocyte or the osteochondral graft transplant does.
And so, you know, there are some technical challenges. You asked me about another challenge we have with this procedure, is we’re trying to build this in and trying to really figure it out. Is - is the issue of - of what you do with a deformed humerus and glenoid. And in those cases, doing it arthroscopically may not be the optimal way because you just can’t reach where you need to go to correct the deformity, and so I’ve started to move now into open procedures with larger grafts and so on. So, there are some things we need to work out. The other thing is we don’t know how long these last, and I think that’s another really big point. But if it reflects what’s been seen in the knee with reasonable 10 and 15 year survivorship, then, you know, I think we’ve done these younger patients a real service.
Why is this procedure new? It’s new because - it’s new and old. I mean I’ll tell you, it’s built upon decades of research in the knee literature where fresh osteochondral grafting, which is what this procedure is about, taking a fresh osteochondral graft, and transplanting it into the shoulder, has been done in the knee since the 1970s. And there’s a lot of data on that and a lot of research that has gone into that. What we’re really doing is trying to take the patient who is younger, you know, typically below 50 years of age - oftentimes in 20s and 30s - that has significant osteoarthritis or a chondral loss, whether focal or global, and we’re trying to transplant the cartilage that they’ve lost in the shoulder joint. And that concept is - is somewhat new in the sense that arthroscopically, we’ve - I’ve developed a technique to do it arthroscopically and, on top of that, as a bipolar graft - both of the socket and the humerus. So in this case, it’s - it’s novel in that technique. Other guys have done this procedure, such as JP Warner and Brian Cole, as a unipolar graft, meaning only the humeral head, as an open procedure, and I’m just building on their work.
Well the benefit of a surgery like this is, in theory, to have an outpatient rotator cuff sparing procedure that eliminates the need, we hope, at least for a time, for metal and plastic prostheses, such as a total shoulder replacement or partial shoulder replacement, and transplant with biological living tissue, such as cartilage, which is what usually the issue is in that patient’s shoulder - they’ve lost cartilage.
I can tell you I’ve been doing this for almost two years now. And there are a couple of hurdles, and it’s a learning curve - somebody’s got to do it in order for us to develop the - the, you know, the solution, so to speak. But you know, one of the hurdles that I’ve learned the hard way is - that is - the question - answering the question of what size graft is enough graft to cover the ball and socket joint adequately to address the symptomatology. And what I found in the early work so far is is that while the grafts really don’t fail - I’ve not had a problem with graft failure when we follow up with MRI scan. What I have seen in some patients is, the larger bone patients, the 30 millimeter grafts that we were initially doing and still do, are just simply just not enough graft. I’ve had the opportunity to scope the shoulder after that and have seen that there’s, you know, just not enough coverage. And so the question is what is the right size? And that’s something that’s going to be worked out over the next decade, I’m sure. But, you know, we’ve moved into this direction, and I think this is a very important move for the field.