
Basal Cell Carcinoma Excision from Lower Lip with Keystone Flap Reconstruction
Main Text
Table of Contents
Maintenance of intact skin throughout the body is essential to prevent dehydration, as a barrier to infection, allow unrestricted movement, and to provide a normal appearance. A flap is a piece of body tissue, usually skin and fat, that always has its own blood supply. Therefore, a flap can be moved anywhere it can reach without worrying about the circulation present at the place that needs it, which is called the recipient site. When compared with all other possible choices, a flap best meets all the requirements for any area needing skin replacement. The keystone type flap as one such option is so named because its design has the shape of the keystone of a Roman arch. If taken from loose tissues adjacent to a defect, it can be simply cut and advanced for any necessary skin coverage. Direct closure of the donor site where this flap comes from is possible so that usually a quite good overall cosmetic result is also obtained. These virtues are shown as an overview in a video where a keystone flap is transferred after removal of a common basal cell skin cancer from the lower lip.
This elderly woman presented with a long-standing, neglected, ulcerated, and oozing biopsy-proven basal cell skin cancer of the portion of the lower lip below the red vermilion. Since larger than 2 cm in diameter, this would be a high-risk type of basal cell skin cancer,1 so surgery would be the standard of care by a wide excision to try to remove all tumor cells. The specimen is always reviewed later under the microscope to check all edges for any remaining tumor. If negative or no tumor is seen, the chance of cure approaches 100%. If not removed surgically at all, or if the edges still have tumor present, a basal cell cancer will continue to grow and eat away to destroy the entire lower lip. Only for the extremely elderly or patients with other medical problems who would not tolerate anesthesia would non-surgical treatment with radiation therapy be an alternate consideration.1
An operating room was used so that the patient would have a “twilight” sedation to make her pain free and comfortable. To summarize the procedure seen in the video, an area extending about 10 mm into normal tissues all around the tumor was marked. This margin was cut all the way down to the muscles of the lip and then peeled off below the tumor to make sure the undersurface was tumor-free. A keystone flap was chosen to fill the hole so created, and that was outlined in the shape of a keystone on the lower chin. The flap borders were cut on all sides until it could be slid upward to not just fill the hole where the tumor had been but to be loose enough so that the red part of the lower lip would not be pulled downward. Because her neck skin was loose, this could be advanced upwards to help close the donor site where the flap had come from.
Another option always possible is to use skin grafts, but these always shrink in time and risk pulling the lip downward so she would be constantly drooling. In addition, since a skin graft is paper-thin, once healed, there would be a conspicuous crater in her chin.2 These potential bad outcomes were prevented by instead using a keystone flap as we did, which gives a superior appearance even though some scars are left.3 This choice proved to be simple to perform in less than an hour with almost no blood loss, so the surgery can be done as an out-patient to allow the patient to go home soon afterward.
Basal cell skin cancer is the most common type of cancer in humans.1,4 As a matter of fact, every year the number of newly diagnosed basal cell skin cancers exceeds the number of all other cancers combined.1,4 Often, they may first appear as a non-healing or bleeding sore (i.e. Figure 1), but many subtypes with different appearances exist so that a physician should be seen to help make the correct diagnosis. Risk factors include fair skin, the extent of sun exposure, use of tanning beds, age over 40, and sometimes genetics.4 Prompt treatment will decrease the amount of skin that has to be removed, most often requiring but a few stitches to close things up. Therefore, the amount of scarring will be less, which for many will be important as 85% do occur in the head & neck region.4 High-risk lesions include large or deep lesions as in the presented case or recurrent lesions that have grown back for whatever reasons.1 As such, more tissue must be removed to obtain a cure, sometimes requiring other approaches5;and then oftentimes a skin graft or flap will be necessary to allow skin healing.
A keystone flap is a trapezoid-shaped local flap from adjacent to a given defect that requires skin replacement.6 It typically consists of skin, fat, and the deep gristle or fascia above the muscles, with its blood supply coming from small branches passing out of the muscle that then pierce through the fascia. The design not only should be over a muscle to ensure adequate circulation but in the loosest tissues that allow the flap to be advanced into the defect while still permitting suturing the donor site closed as well (i.e. Figure 2). All borders are cut down to near the fascia, or deeper as needed to the muscle, to make the flap loose enough to stretch into the defect. Once reaching the farthest edge of the wound, all sides are sewn together to complete the repair (i.e. Figure 2). The area can be washed with soap and water within a day. Activities would be restricted only to ensure that tension on the sutures is avoided. They are then removed usually within 2 weeks to leave a nice result.
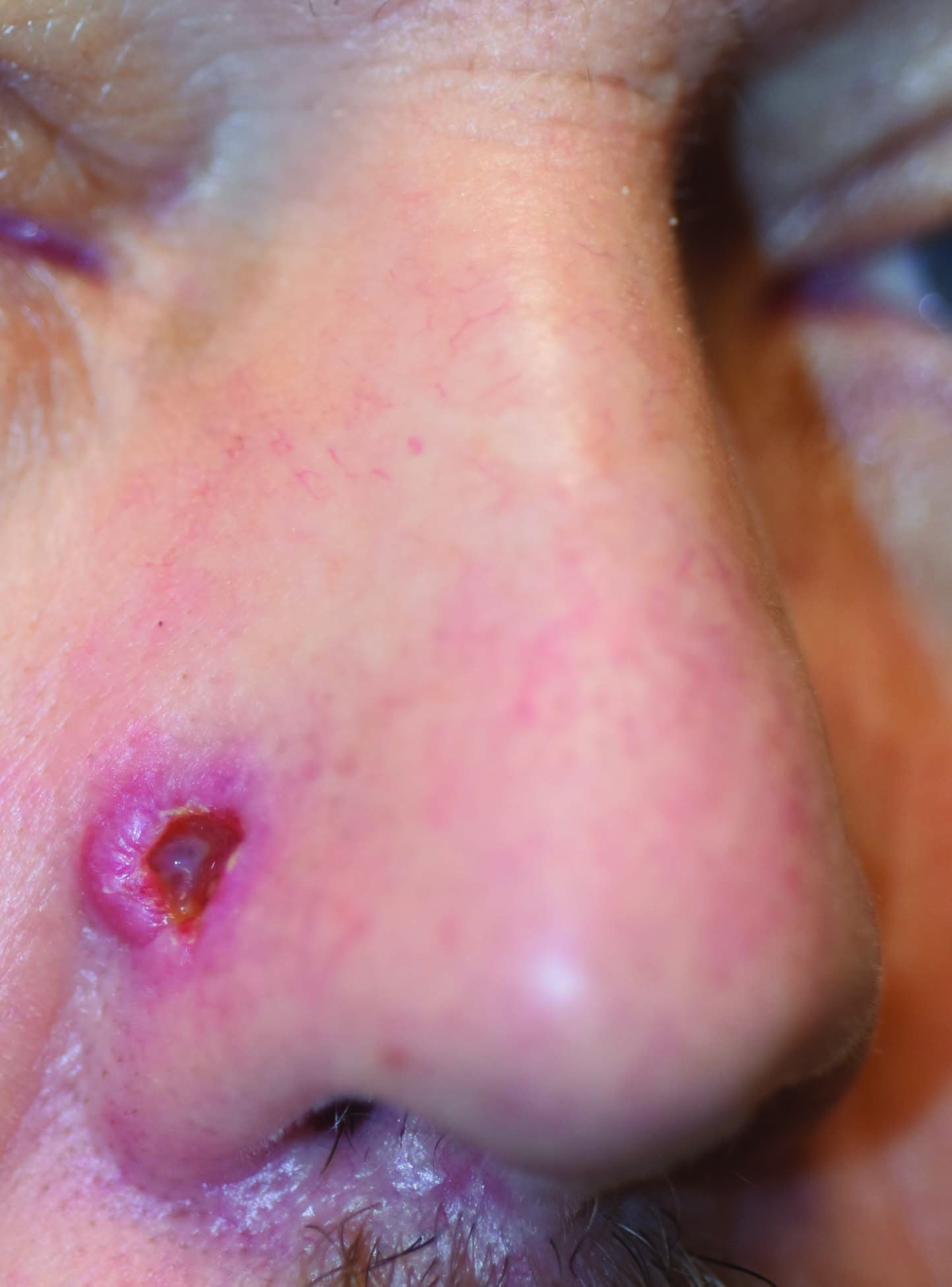
Figure 1. A common type of basal cell skin cancer is called “nodulo-ulcerative”, since it looks like a raised nodule or bump with a hole or ulcer in its center.
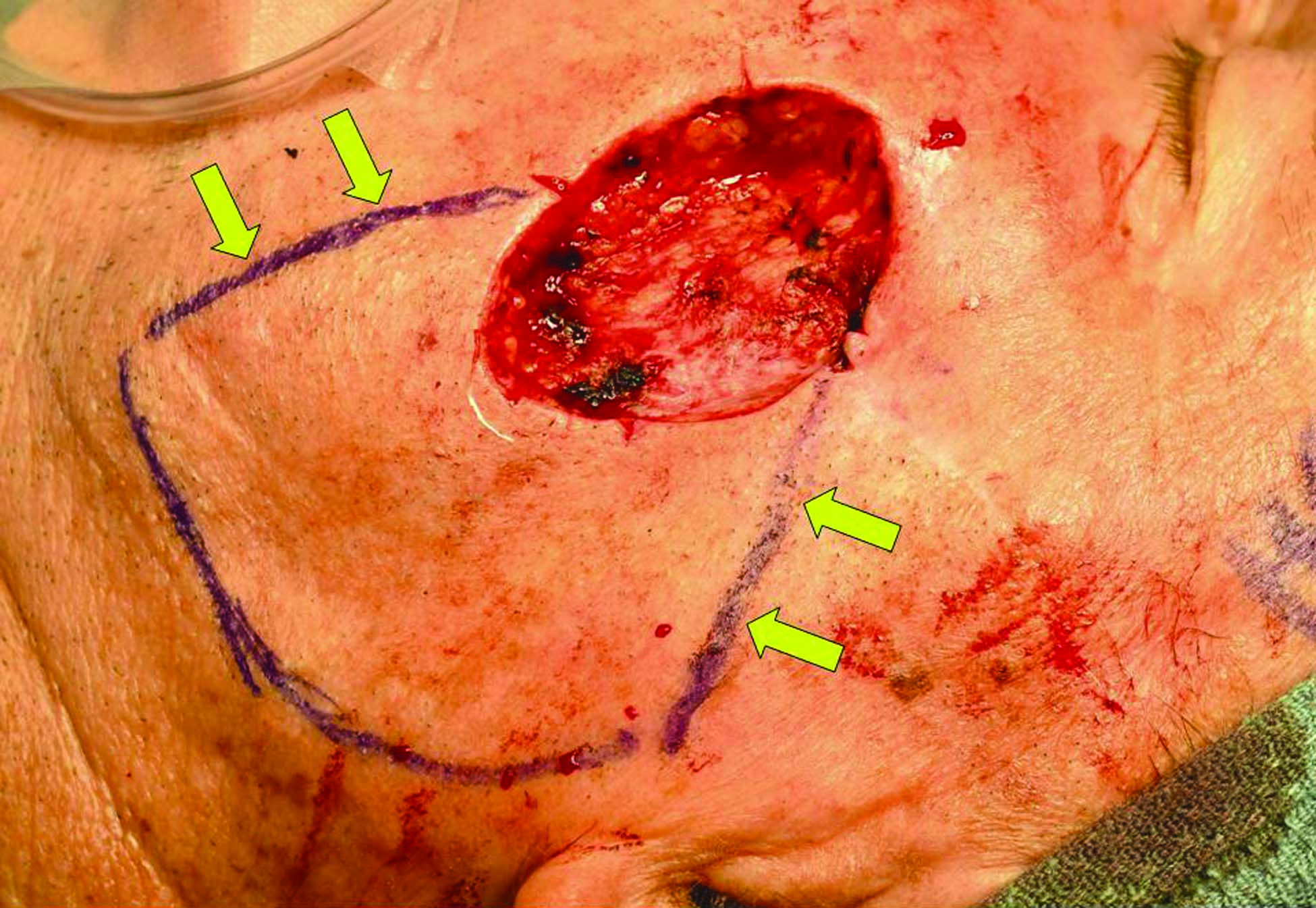
Figure 2A. The open crater can be seen following basal cell skin cancer removal from the left cheek, with the keystone flap design below. Tangents on either side of the defect [arrows] are drawn toward the loose skin of the neck. Their length must be equal to the height of the defect, with a curved line or arc joining them to make a trapezoid.
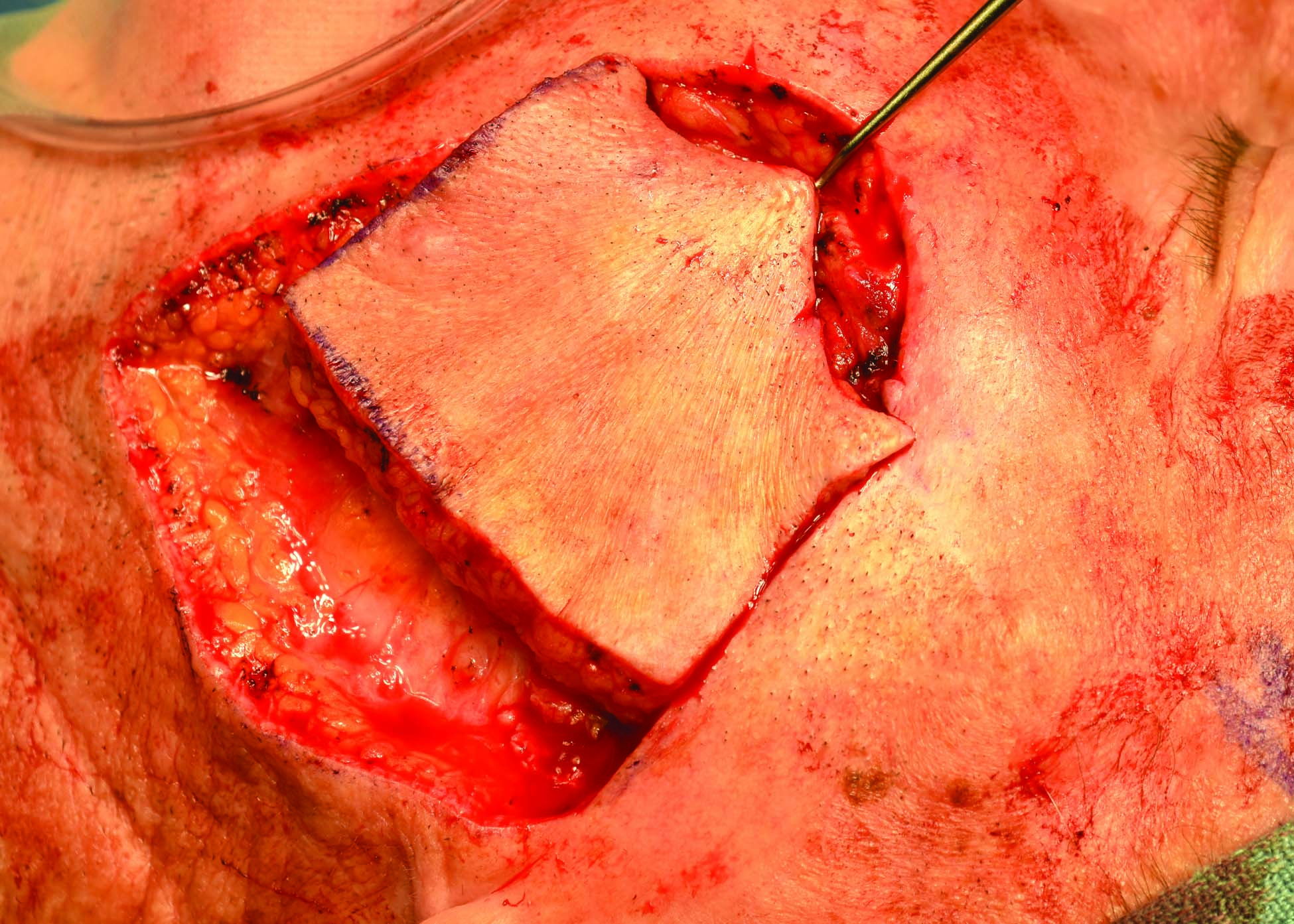
Figure 2B. The 3 marked sides of the flap are cut down to near the fascia until the flap can be advanced superiorly to the farthest edge of the wound.

Figure 2C. The neck skin is then drawn up into the cheek to allow all sides of the flap to be sutured in place to thereby close all areas.
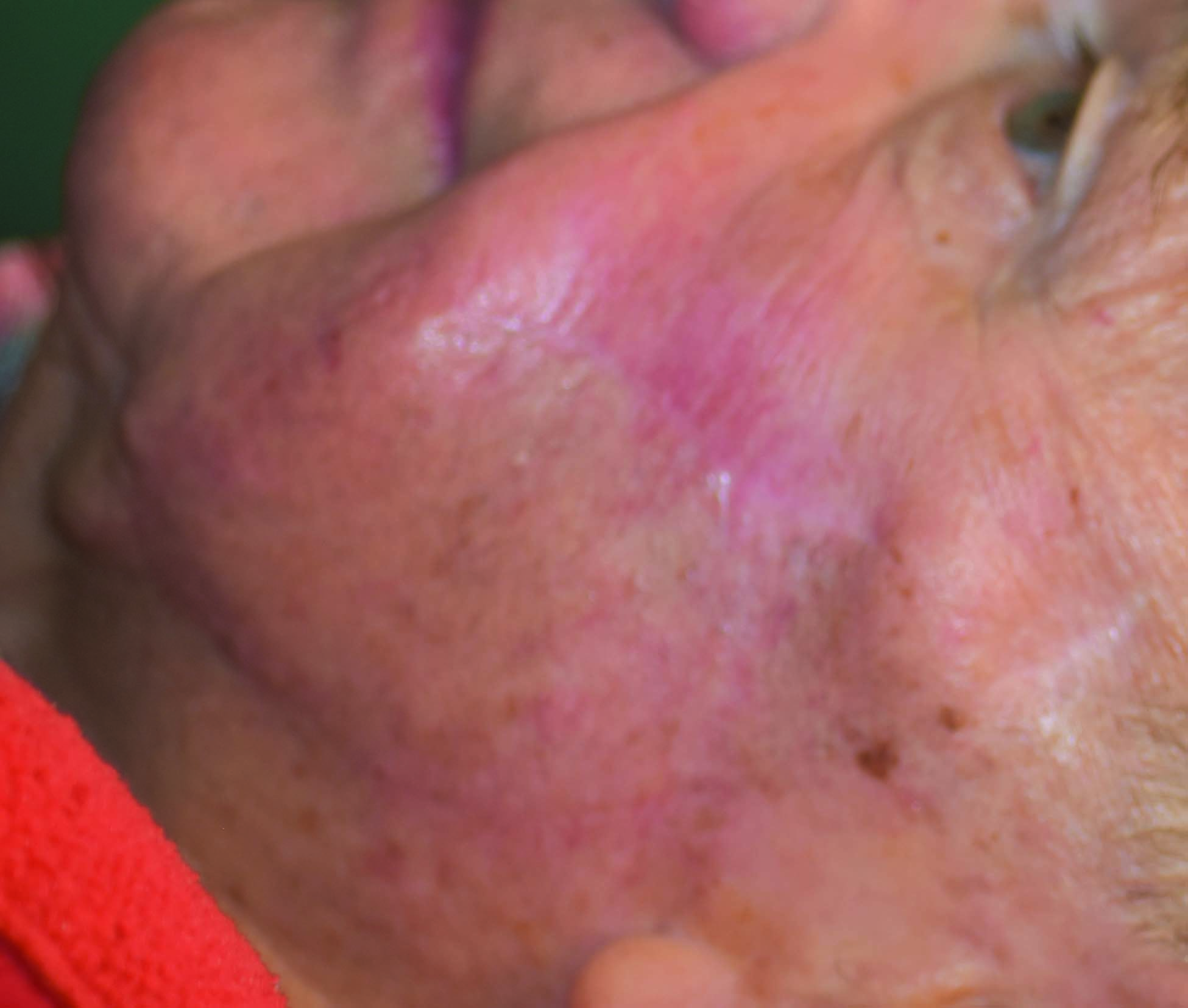
Figure 2D. Final scars of the left cheek are barely seen 3 months later.
Nothing to disclose.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Kate Mertz, Surgical Technician, from Bowmanstown, Pennsylvania, was the first assistant for all surgery.
Citations
- Mendez BM, Thornton JF. Current basal and squamous cell skin cancer management. Plast Reconstr Surg. 2018;142(3):373e-387e.
- Hallock, GG, Morris, SF. Skin grafts and local flaps. Plast Reconstr Surg. 2011;127:5e-22e.
- Stone JP, Webb C, McKinnon JG, Dawes JC, McKenzie CD, Temple-Oberle CF. Avoiding skin grafts: the keystone flap in cutaneous defects. Plast Reconstr Surg. 2015;136(2):404–408.
- Gulleth Y, Goldberg N, Silverman RP, Gastman BR. What is the best surgical margin for a basal cell carcinoma: A meta-analysis of the literature. Plast Reconstr Surg. 2010;126(4):1222-1231.
- An Introduction to Mohs Micrographic Surgery. American Society of Dermatologic Surgery.
Access: https://www.youtube.com/watch?v=W5Paup_-S4A&feature=youtu.be. 2017. - Behan FC. The keystone design perforator island flap in reconstructive surgery. ANZ J Surg. 2003;73(3):112–120.
Procedure Outline
Table of Contents
- Approach
- Incisions
- Mobilization
- Reconstruction
Transcription
CHAPTER 1
I'm Dr. Hallock. Today we're going to talk about ways to close skin wounds using various methods. And this case is an elderly lady with a basal cell carcinoma of the lower lip. We're going to try to close the wound so we do not cause an ectropion, or an eversion, of her lower lip, pulling it down, as well as possible. And at the same time, avoid doing a skin graft, which would be from a cosmetic standpoint an inferior way I think of taking care of something on somebody's face. To do this I'm going to take advantage of the fact that she is elderly, she does have a lot of loose skin, particularly in her neck that we can advance upwards by creating a flap below the defect where we removed the tumor, and then we take a flap and pull the skin upward. And what I'm doing a lot these days is what's called a Keystone flap. A Keystone flap looks like a trapezoid, which is the stone that holds up a Roman arch. I'm sure you're all familiar with that. So the flap has the shape of a Keystone. It is marked with the upper, or lesser curvature of the Keystone, the same as the lower part of the defect you're going to reconstruct. You cut all the sides. You then advance it upwards. It survives because the blood flow is through tiny blood vessels beneath it, which you have to carefully protect. But because of her skin laxity you'll be able to advance this to close the defect as you will see. This is a very versatile means of reconstructing soft tissue defects in any part of the body. It could be applied to anywhere where there's enough skin laxity to allow this to be done as we're going to show you. A keystone flap, you start off by drawing a tangent on the opposite sides of the width of the defect. You make the tangent a line that extends the length of the will be the width of whatever the defect is. Draw those two lines. Then you connect the two with a larch arc to complete a trapezoidal shape that looks like a Keystone of a Keystone arch. The next step is to cut the three lines that you we've now drawn - the two tangents and also the arc that joins the two tangents. You cut them, I usually go down in the subcutaneous tissues to the equivalent of what we all know as Scarpa's fascia, but if you go to the underlying muscle that might be there, that's perfectly fine. If you undermine the deep fascia just above the muscle, that's perfectly fine to do that as long as you're careful enough to keep enough contact with the underlying muscle so that there is some blood supply to the flap. At this point the flap should be mobile enough that you can then pull it upwards to close your defect by sewing it first to the upper end of your defect. Now, if that's not true, then sometimes I will undermine the leading side of the flap or the end of the flap, whatever's necessary so I get enough reach to what I'm going to do. Once I have enough mobility in the flap I'm then able to close the wound. The first thing I do is I take the lesser curvature of the keystone flap and that will correspond to the border of the defect that the flap is next to. I will take that and I will then bring it up to close the opposite side of the defect. I usually put a few subcutaneous sutures in that are absorbable to provide long-term strength to my closure. And then I will close the skin at this level first. Following that, I will close these tangents to the sides of the defect. And then ultimately, I will place a stitch in the center of the greater curvature of the flap and the donor site itself, where it came from. Tie that suture, and that will set up where I'm then going to close the lower part of the Keystone flap in a similar fashion, although I don't put any subcutaneous sutures in. This will leave a few openings where the tangent side is to the flap. That represents the amount of tissue that you advanced the flap past. And those openings can be closed with a few simple skin sutures to complete the repair. I would say the keystone flap has great versatility in every part of the body. You must make sure that you design your flaps in an area where the skin is elastic enough and flexible enough that you can then advance the flap. For example, if you design it over the tibia in the lower extremity, it's not going to have enough flexibility to be advanced. You should avoid that. You should also make sure that you have enough blood supply coming to the flap from its under-surface, that's where it gets its blood supply. Therefore the flap really has no role in the scalp because underneath the skin and fat in the scalp is the skull, and not little blood vessels that are going to the overlying tissues from the skull. So that's probably the only place in the body that I would say this probably should be avoided in doing this flap.
CHAPTER 2
What we're doing today in this lady is treating her for skin cancers, which is a very common problem in Honduras. This lady has multiple ones. I'm just going to show you two different approaches to taking care of the problem. The first thing, this is your typical basal cell carcinoma that we see here. The important thing is to get all the tumor out, get all the roots out. So the first thing you want to do is to make sure you have margins that are free of tumor. So we're going to go, here's the tumor here, you see this red area, little ulceration there? We're going to go into normal skin. In this case I don't have frozen section control so I'm going to take about a 5 mm margin around it in all directions. Going into normal skin. You see how I'm going around all the area that's red? Okay, so that should be negative margins. Now this patient's under general anesthesia so we don't need local anesthesia here. But I'm going to put it in anyway, and that's because we have epinephrine with this. Epinephrine is a vasoconstrictor and it will cut down the bleeding that we have. So, a little epinephrine. I like to wait about 7 minutes or so to get enough of an effect that it will cut down my bleeding. I'm also injecting the area that I'm going to close this because although I could do a skin graft to close the hole I'm going to leave when I remove the cancer, a skin graft on the face does not look pretty. And as a plastic surgeon we're also interested in - not just getting rid of the cancer, but also making it look good for the patient afterwards. So she has lots of loose skin that will allow me to move skin from someplace where she has more than enough to fill in the hole. And that we'll see as we go along. Okay, we've waited enough for the epinephrine to take effect, I think you can sort of see the skin has turned white around there so we're about ready to start here.
CHAPTER 3
Normally I do this with suction, but we don't have that luxury here in Honduras, so I'm going to go widely around this. Take all the cancer out. Do we have a suture to mark this then? Is there a suture on board? 4-0 nylon, PS-2 please. Hopefully black. So actually it's not bleeding very much.
CHAPTER 4
Okay, so what I'm going to do now is of course we send every specimen goes to the pathologist to examine to make sure all the tumor is actually gone. We cannot do that right now, but I'll take a suture please. And I'm going to mark the specimen. And if you look at the face as a clock, the head will be 12 o'clock, the top of the head. So I'm going to put a suture in at the top of the specimen. I will call this a 12 o'clock margin. This is the 12 - and that will allow the pathologist to orient the specimen when he examines it to make sure the whole tumor is gone. And if not, you have to go back and take more wherever it's still present. We cannot do that here today though.
CHAPTER 5
Next step is to remove the cancer. I'm going to go real deep here because I want to make sure I have it all out. We use a Bovie to stop the bleeding, but also to do the dissection. Just looking at that grossly to me, I'm getting deep enough. This is very superficial. So I think I'm getting around it nice and we're almost done. Of course, you can do this with a knife if you want, but that tends to be bloody. So there we are. Specimen's all removed. It's marked at the 12 o'clock margin. We have hopefully all the cancer removed. So now I have a hole. How am I going to close that? You see that if I brought the chin up like that and brought the lip together the closing of the sutures, then you have - the mouth is going to be open, so that's not a good solution. See how the lip is pulled down? That's not a good solution to close that. Instead we're going to do what we call a flap. I could put a skin graft on this, but you'd have a big cavity there, it would look horrible. Instead I'm going to actually move the chin up, but I'm going to do it as a flap. I'm going to mark that now.
CHAPTER 6
In this lady, she has lots of extra skin in her neck, so I can take some of the - because she is 97 years old, I can take some of that extra skin. 97. And I'm going to do what's called a Keystone flap. And that is done by marking a line. Can I have the marker - the ruler please? I'm going to find the left and right sides. I'm going to mark the left and right sides of the defect I have. Going to measure the height of it, which is about 2 cm, so I'm going to draw, along this tangent here, I'm going to draw a 2 cm line. I'm going to do the same on the other tangent. Then I'm going to connect them. With a large curved arc. So if you look at that carefully, that looks like if you look at a Roman arch, the sides of the Roman arch, there's this stone at the top of the Roman arch that holds it up, that's called a Keystone. So this looks like a Keystone, and we call this a Keystone flap. The blood supply to this flap will be coming from the bottom, so I can cut it at all sides, and it will still live. Theoretically. Let's find out.
So now I'm going to cut the 3 sides of my Keystone flap. And remember, I've infiltrated this with epinephrine already. And - one more. Okay.
All right so, you can go - when you do a keystone flap, you can actually go all the way down to the muscle underneath, and it will still live. But I usually don't have to do that to get enough mobility of the flap to move it up. Wait, come down here and hold that back there. I want to make sure I don't have any bleeding here that's excessive. Okay, we'll march all along. I'm making sure now that I have all the bleeding stopped on the edges of my flap. And I want you to pull up on the flap now. Just put your skin hook there. And, it's still a little tethered here, so I'm going to undermine a little bit back here on the greater curvature of the flap. And let's go and do the other side too. Just freeing it up a little bit. Okay, that's good. I'm just making sure there's no bleeding. Okay, so here's the flap. We're going to move it up like that. See how that does not distort the lip? We'll find out what happens now when we suture this closed. I just want to check this one more time. Make sure I don't have any bleeding. I want to make sure there's no tension here. I do not want a lip ectropion. Okay.
So, my next step is - when I do this is I want to - this is the lesser curvature of the Keystone flap, and I'm going to advance it up to the superior aspect of the defect. So I'm going to go in the center - and just put a stitch in so I can help orient myself. I'm going to go in the center of the flap, the center of the defect. And there we have it. It is coming down a little bit, but we'll compensate for that in a minute. And, we'll take the… Now, after I do that I like to put in a couple of subcutaneous, absorbable sutures in. So I don't rely only on my skin closure here because I want to take some of the tension off of the flap with a - with a subcutaneous suture. Okay. Put in as many as you feel comfortable in doing. I put in at least 1 in on either side of my first suture. Okay, so once we've done that our next step is to close the lesser curvature of the flap into the defect. I'm going to do that with 4-0 nylon, that will be next. I don't like to invert the skin. The first stitch was a simple stitch so I'm going to put the - I'm going to put vertical mattress in just so I don't invert - I don't want to invert the skin, I want to evert it, so I get a better closure for better healing. So I'll try to do that. So there I have epidermis to epidermis. I've everted the skin, whereas the simple stitch like I put the first one in, you tend to invert and you don't get skin to skin. You get better healing this way. Kate, I'm going to probably do both sides of this. Actually, you probably do the other side, once we get this set up. I do have a little bit of eversion of the lip - that in time will stretch out I think. So lots of suturing with the Keystone flap. There's lots of suturing, so this is very - but it's important. I think I've gotten - that side is pretty much done. Maybe one more. The Bovie's about to hit the deck here, guys. Okay. So this is a flap. How is a flap different from a graft? A graft, whether it's skin, or nerve, or tendon, or cartilage, or bone - a graft has no blood supply to it. It relies on where it's put to heal - to get new blood vessels in it. This is a flap, it has its own blood supply at all times. If I push on this, see it's white? And then you get capillary refill? That blood is coming in. That shows you that in spite of my cutting it all the way around it's still getting blood supply. It's still alive. It's a flap. And I think by putting this here she'll have much better ultimate appearance to the area too, and I don't have to worry about the graft taking, because this is all alive constantly. Oops, I'm going to have to redo that one. As I always tell the - junior doctors, never use the word "oops" under local anesthesia. It makes the patient very nervous. Let's do that one again. Yep. We're almost there, step 1. Okay. Okay, the next step is to close the sides. I want to advance my flap up as much as I can, so what I will do is - it's easy just to close side-to-side. By the way, see the bleeding - you see the bleeding there when I stuck that with a needle, implying that there is blood in the flap of course as we all know. So what I'm going to do here is I'm going to - I want to pull my flap up as far as I can and not just go side-to-side. That's the easy thing to do. So I want - I'll move my flap up as far as I can, so I'm going to take a shorter bite on the chin skin, a bigger bite on my flap skin. We're going to pull that up. Kate, what I think I'm going to do is I'm going to throw a stitch on the other side, and then you can start doing the same, okay? All right, smaller bite here, bigger bite on the flap. All right, Kate, you get that? You get a smaller bite here, bigger bite there, and that will pull - that pulls the flap up because we do have a little bit of ectropion. See how that's coming down? We're going to try to minimize that. Kate, why don't you go ahead and start closing the other side there, make things easier. I don't have to put a vertical mattress every suture, so I'm going to cheat here and put a simple in. Okay, please. I cannot get any more suture out of that. Okay. We always think green - to save. So, bigger bite on the flap than on the non-flap side. So I actually use - I use this flap everywhere in the body - except for the scalp, because it relies on little tiny blood vessels coming underneath it, and on the scalp, underneath the skin on the scalp is the skull of course, so there are no blood vessels coming in there to keep it alive, but this flap can be used anywhere in the body, otherwise from head to toe. And I use - this is probably the most common flap I'm using today to take care of skin cancers - because it's easy and it's versatile, and you can use it anywhere. We've essentially got that closed up. Now I got to close the greater - this is the greater curvature of the flap, the larger one. And here, I know this will go about right like that, right? And so I'm going to go in the center of this, and then I'll go - coming up on the center of the flap, and that advances the neck skin in to close the donor-site deformity. So I'm pulling the neck skin up, and that will close where the skin of the chin came from. And I do not put subcutaneous stitches here because I think that restricts advancement of the flap. All right, let's finish this up. Let's do it. So lots of - when you're doing a Keystone flap, lots of suturing. It's really not very exciting because you have to do a lot of suturing. A skin graft's a lot easier to do, but I think this gives you a better - will give her a better appearance. This whole concept comes from one of my friends who lives in Australia actually, Dr. Behan. He came up with this idea. He lives in Australia, he's really from New Zealand. And as with most things today with the internet and what have you, it's amazing how information can be transferred around the world almost instantaneously today. And most plastic surgeons now all feel comfortable doing this procedure. Just throw a couple down here and then - we will leave a - Yeah, I'm going to show you that there's one more step in the donor site you have to do besides doing this that's characteristically necessary. We're almost done. Notice that we're almost finished here and the flap has nice pink color to it so we're not compromising blood flow to the flap by doing this. And the lip is everted a little bit, but I think she'll still be able to close her mouth. Okay, so now, notice that we have an opening. There's an opening on either side here where we advanced the flap up, and there's an opening here. Same is true here, on both sides. So really, I think the Keystone flap is like a double, opposing V to Y advancement flap. It's just two V to Y advancement flaps that are coming together. And we're going to close this, where we advanced the flap - we're going to close this like we would close it at the Y-portion of a V to Y advancement flap. So that's what I'm going to do here, just throw one stitch here on both sides. It'll be good. Kate, you can do the same thing. Just - you want to close that to that with a - vertical mattress, that would be good. And that will com- and we have one final step to do after we finish this part. We're almost home. How you doing? That's all right, just pull it, just pull it, just - you got it? Okay. Okay, here we go. All right, one last step is when I advanced the flap - we have a little bit of extra triangles of tissue superiorly that I did not sew in. You probably noticed that. See how it sticks up over the edge? It sticks up over the edge. I'm going to trim those back so it's flush with the normal skin. So I'm just going to trim those around. So I can close that off. And this is the way plastic surgeons are, they're very obsessive. They get things where they want them. I can get - I do a lot of microsurgeries so for me, this suture is long. Oh my goodness, that suture is - I can get 5 stitches out of that. And that will complete our repair I believe. We'll get the patient to massage the flap constantly in the postoperative period to pull it up. To pull it up - it will stretch. It will stretch. Yeah, that's fine. All right, there you go, Keystone flap.