
Transperitoneal Laparoscopic Right Adrenalectomy for Cortical Adenoma
Main Text
Table of Contents
Primary hyperaldosteronism, or Conn's syndrome, is a disease in which one or both adrenal glands produce excess amounts of aldosterone, leading to hypertension and hypokalemia. Common conditions resulting in this disorder include adenoma of the adrenal gland or hyperplasia of both adrenal glands. In rare cases, it is caused by malignant growth in the adrenal cortex or familial hyperaldosteronism. High blood pressure may cause headaches or blurred vision. Low potassium may cause fatigue, muscle cramps, muscle weakness, numbness, or temporary paralysis.
Primary hyperaldosteronism is diagnosed by measuring serum levels of aldosterone, renin, and potassium. Patients classically have high aldosterone levels, suppressed renin levels, and low potassium levels. Once the diagnosis is established, the localization of the source is performed using imaging studies. Adrenal vein sampling is also performed to determine more precisely and directly the side that is producing excess aldosterone.
Primary hyperaldosteronism caused by an adrenal gland tumor is treated with adrenalectomy. Approximately 95% of patients will notice a significant improvement in their hypertension after successful surgery. Here, we present the case of a 58-year-old female with hypokalemia and long-standing hypertension refractory to medical treatment. Her blood tests showed high aldosterone levels and low renin levels, confirming the diagnosis of hyperaldosteronism. On CT scan, an adrenal nodule was noted on both sides. Adrenal vein sampling identified the right adrenal nodule as the cause. Laparoscopic access was gained, the adrenal gland was dissected and exposed, the adrenal vein ligated, and the adrenal gland was removed.
Primary aldosteronism was first described by Jerome Conn in 1956.1 The syndrome that bears Dr. Conn’s name is characterized by hypokalemia and hypertension, both of which are relatively refractory to medical management. Primary aldosteronism is a common, though underdiagnosed cause of secondary hypertension. Between 1–10% of patients with hypertension are thought to have underlying primary hyperaldosteronism.2
The most common causes of primary aldosteronism are primary aldosterone-producing tumors or hyperplasia of the zona glomerulosa of the adrenal gland.3
For patients with medication-resistant hypertension, a workup for Conn’s syndrome is indicated. If a unilateral tumor is identified as the source of the excess aldosterone, surgery to remove the tumor is indicated.
The patient is a 58-year-old female with long-standing hypertension. She had been treated with three medications with no satisfactory relief of her hypertension. Her laboratory examinations were notable for long-term hypokalemia, with her lowest recorded value being 2.3 mmol/L (normal range 3.6–5.2 mmol/L).
Her serum aldosterone and plasma renin activity (PRA) were measured to determine her aldosterone-to-renin ratio (ARR). Her serum aldosterone was 24 ng/dl, and her PRA was 0.6 ng/ml/h, giving an ARR of 40 (range of normal < 30 ng/mL/h).
After the CT scan showed bilateral adrenal lesions, adrenal vein sampling was performed to measure aldosterone and cortisol levels, and to determine their ratio using the inferior vena cava as the control (Table 1).4 The aldosterone levels in the right and left renal veins were 3,800 ng/dl and 78 ng/dl, respectively. The control value from the inferior vena cava was 66 ng/dl. Based on these values, including cortisol measurements, the calculated aldosterone/cortisol ratio of right vs left was 13.75. Any ratio over 4 is considered a positive finding. Taken together, the laboratory findings suggest that the right adrenal gland was the source of the excess aldosterone.
Table 1. Adrenal Vein Sampling
.png)
*RT A:C ratio / LT A:C ratio > 4, suggesting that the right adrenal gland was the source of excess aldosterone.
Primary aldosteronism is not characterized by any particular sign on a physical exam. Nevertheless, long-standing hypertension may lead to left ventricular hypertrophy that may generate an S4 sound on auscultation. Other nonspecific signs include carotid bruits, muscular weakness, and mental status changes associated with hypertensive encephalopathy.3
An abdominal CT revealed a 2.6-cm lesion in the right adrenal gland and a 1.3-cm lesion in the left adrenal gland (Figure 1).
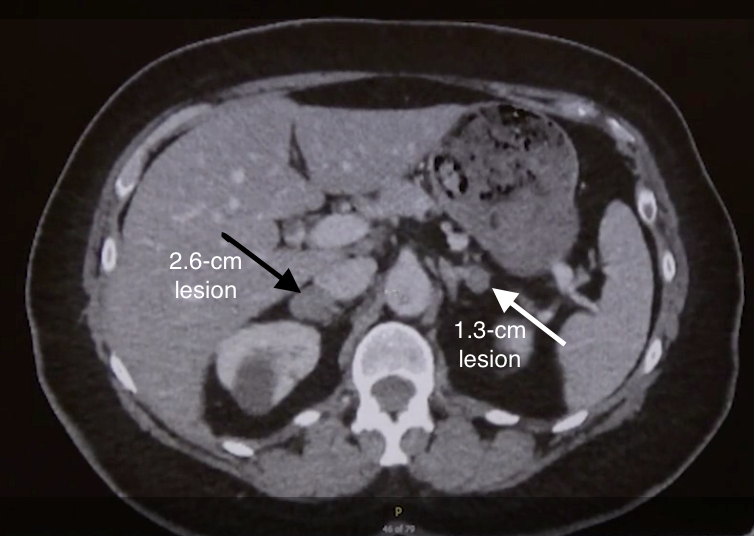
Figure 1. Abdominal CT
Noncontrast abdominal CT revealing a 2.6-cm lesion consistent with a right adrenal mass (black arrow), and a 1.3-cm lesion consistent with a left adrenal mass (white arrow).
Left untreated, the course of primary hyperaldosteronism is characterized by sequelae of hypokalemia and chronic hypertension. Muscle weakness and elevated serum creatine kinase levels secondary to hypokalemia have been reported as a presenting symptom and sign.5 Chronic hypertension places patients at greater risks of major adverse cardiac events, including atrial fibrillation, myocardial infarction, and stroke.3
Laparoscopic resection of unilateral adrenal tumors is the treatment of choice for Conn’s syndrome.6 However, some patients will be managed successfully with antihypertensive medications. Surgery is generally contraindicated in patients with bilateral disease; such patients are best managed medically with antihypertensive agents, including mineralocorticoid antagonists. The surgical approaches are primarily laparoscopic or retroperitoneoscopic.7
The goals of treatment are to reverse the patient’s hypokalemia and hypertension. The procedure reverses hypokalemia in virtually 100% of cases. However, patients are able to discontinue antihypertensive medications in only 35% of cases, though the degree of hypertension generally diminishes.8
Unilateral adrenalectomy is most effective when the disease is unilateral. Patients with bilateral hyperplasia or bilateral aldosterone-producing tumors (very rare) are generally not candidates for surgery and should be treated medically with blood pressure-lowering medications and aldosterone-blocking agents such as spironolactone.
Using a laparoscopic approach, we removed a 2.5-cm cortical adenoma from a 58-year-old woman with primary aldosteronism. One feature of this case worth noting is that the patient had evidence of bilateral tumors on CT; however, adrenal vein sampling suggested that the right-sided tumor was the source of her excess aldosterone.
We now, generally, send patients home the day of surgery (outpatient), provided they have no significant comorbidities. They are advised to continue to monitor their blood pressure at least twice per day and to take their blood pressure medications as prescribed (we usually cut down significantly on the number of agents and dosing). After discharge, we follow up closely with telephone calls later the same day and the following day.
This patient was discharged on only her beta-blocker. In the follow-up, we monitored her blood pressure and potassium levels. The goal with this patient was to wean her eventually off of all blood pressure medications.
- Endo Paddle
- Endo Catch Bag
None.
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Conn JW, Louis LH. Primary aldosteronism, a new clinical entity. Ann Intern Med. 1956;44(1):1-15. doi:10.7326/0003-4819-44-1-1.
- Piaditis G, Markou A, Papanastasiou L, Androulakis II, Kaltsas G. Progress in aldosteronism: a review of the prevalence of primary aldosteronism in pre-hypertension and hypertension. Eur J Endocrinol. 2015;172:R191-203. doi:10.1530/EJE-14-0537.
- Cobb A, Aeddula NR. Primary Hyperaldosteronism. [Updated 2019 Apr 21]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539779/?report=classic.
- Deipolyi A, Bailin A, Wicky S, Alansari S, Oklu R. Adrenal vein sampling for Conn’s syndrome: diagnosis and clinical outcomes. Diagnostics. 2015;5(2):254-71. doi:10.3390/diagnostics5020254.
- Olt S, Yaylaci S, Tatli L, Gunduz Y, Garip T, Tamer A. Hypokalemia-induced myopathy and massive creatine kinase elevation as first manifestation of Conn's syndrome. Niger Med J. 2013;54(4):283. doi:10.4103/0300-1652.119658.
- Kim K, Kim JK, Lee CR, et al. Surgical outcomes of laparoscopic adrenalectomy for primary hyperaldosteronism: 20 years of experience in a single institution. Ann Surg Treat Res. 2019;96(5):223-9. doi:10.4174/astr.2019.96.5.223.
- Wierdak M, Sokołowski G, Natkaniec M, et al. Short- and long-term results of laparoscopic adrenalectomy for Conn’s syndrome. Wideochir Inne Tech Maloinwazyjne. 2018 Sep;13(3):292. doi:10.5114/wiitm.2018.74833.
- Parthasarathy HK, Ménard J, White WB, et al. A double-blind, randomized study comparing the antihypertensive effect of eplerenone and spironolactone in patients with hypertension and evidence of primary aldosteronism. J Hypertens. 2011 May;29(5):980-90. doi:10.1097/HJH.0b013e3283455ca5.
Cite this article
sonia cohen, Richard Hodin, MD. Transperitoneal laparoscopic right adrenalectomy for cortical adenoma. J Med Insight. 2023;2023(240). https://doi.org/10.24296/jomi/240Procedure Outline
Table of Contents
- Mark Trocar Positions
- Inject Local Anesthetic
- Incision
- Hasson Port Placement
- Insufflation
- Laparoscopic Abdominal Cavity Exploration
- Placement of Ports
- Adhesiolysis
- Mobilization of Right Lobe of Liver Through Division of Triangular Ligament
- Peritoneal Incision and Dissection Towards Psoas Muscle
- Right Adrenal Vein Identification, Clipping, and Division
- Final Check for Hemostasis
Transcription
CHAPTER 1
Our patient today is a 58-year-old female, who has long-standing hypertension.She's been on three medications for a long timeand also has had hypokalemia -pretty significant - with potassiums as low as 2.3.So her primary care doctor didan evaluation and found her to have hyperaldosteronism.Her serum aldosterone was 24.Renin was suppressed at less than .6, so the ratiowas well over 30, which essentially confirmed thediagnosis of hyperaldosteronism. She then had a CAT scan,which you can see here. And -going from above, coming down, you can seethe adrenal glands coming into view,and on the right side, you see this2.6-cm lesion - clearly seen in the right adrenalthat has characteristics of a cortical adenoma.On the left side, there was also a lesion. This was smaller -1.3 cm - again, consistent in terms of imagingfeatures with a cortical adenoma. So, shehad bilateral cortical adenomas by imaging.One was 2.6 cm. The other one1.3 cm - clearly needs adrenal vein sampling.We do that in most cases anyway,but obviously, in this patient,there's no question we need to determinewhich side might be responsible for herhyperaldosteronism.So her adrenal vein sampling was done, andthe results were very -very clear-cut step up on the right side.So her peripheral values of aldosterone to cortisol was66/26. Ratio is 2.5. On the left side, the aldosteroneto cortisol was 78/197 with a ratio of 0.4, whereas onthe right side there was a very marked step up:aldosterone of 3800 witha cortisol of 692. That ratio was 5.5. So when we do the ratios right:left,the aldosterone:cortisol - 5.5 over the left side, 0.4 -the ratio was 13.75 -clearly over 4, which is usually the cutoff we use. And sovery good result in this patientsuggesting that the right-sided adenoma is the onethat's the culprit in causing her hyperaldosteronism.So our plan today isfor a laparoscopic right adrenalectomy.So the key steps for this operation:She'll be in the supine position, intubated, andput under general anesthesia.We'll then put her in a lateral decubitus position -left lateral decubitus position with the right side up.We use a bean bag inflationdevice to make sure that all thebony prominences are well-padded and that she'sin good position.The bed is flexed so that we maximize the exposureto the abdomen.And then I use a right paramedian open approach. So we put theHassan cannula in the right paramedian incision,and then we'll use a12-mm trocar for the epigastrium,and I use an Endo Paddle throughthat port site to lift up the liver.The Endo Paddle works very well for that purpose.And then two 5-mm trocars along the right costal margin to do the dissection.We'll use the harmonic scalpel and mobilize theliver, lateral attachments, and inferiorly, and then basicallycircumferentially dissect out the adrenal gland,dividing the attachments to the diaphragmand retroperitoneal muscles, medially we'll separate it from the vena cava,and then isolate the adrenal vein, which we will clip twice on each side,and then remove the gland completely, place it intoan Endo Catch bag, and bring it out, and then close the port sites.Adrenal surgery is of course not that common,and like any operation it's important tohave experience andsort of confidence to be able to do the operation safely.The risks on the right sidemainly from a technical standpoint have to dowith the vena cava and the short adrenal vein.On the left side,the adrenal vein is longer and of course is comingoff the renal vein, so it's a little bit easier from that standpoint, buton the other hand,the dissection and exposure of the glands is morecomplex because youhave to move the spleen and pancreasout of the way and track them, andso it's a little more difficult to get to the adrenal gland.But, I think this operation in particular -it's not so much the technical aspectsas the sort of pre-op evaluationand making sure that you are doing proper diagnosis andpatient selection especially for something like aldosteronoma,but even other conditions of theadrenal gland - so important to befamiliar with how you establish the diagnosis, whetherit's Cushing's orhyperaldosteronism, and how you determinewhether a patient is going to benefit from surgery.In this particular situation with hyperaldosteronism,obviously, you need to be very confident thatyou're taking out the correct adrenal gland,that it's the side that is producingthe excess aldosterone and is likely to help the patient.The last thing we wantto do is to subject the patient - anybody toan unnecessary operation.
CHAPTER 2
So we're going to - let's see. Here's the -rib margin. Here is her anterior superior iliac crest,or the iliac crest. So,what we're going to do is go paramedian, near the umbo -maybe about here.We want to let, you know, the pannus drop down a little bit,and then we're going toput a 12-mm trocar somewhere here for theEndo Paddle to lift the liver up,and then two 5-mm trocars over there.Do we have the local anesthesia?
You don't want to use the Bovie?You can use the Bovie.You can show people how to use the Bovie.
CHAPTER 3
You just cut - two narrow Richardson's, please.Yeah - maybe... A little bigger?Like by a millimeter. Okay.Yep, so -you want to go that way, and you can hold this, I guess.Can I get a Schnidt, please? Go ahead.This is all the local anesthesia.Okay, just...Okay, hold on.There's white, right?So just a small opening in the anterior sheath - okay, good.We'll take 0 Vicryl.So we'll put a figure of eighton both sides of the opening - longer needle driver, yeah.Let's see, what did you get? You got the upside? Yep.Oh... Now you want me to go...?Yeah, no, you want - you know,a figure of eight on the upside, right? Yep.Hold that up -snap and scissors, please.Look, it's long, It's okay, I don't like the short ones.Let's see, cut that. And then another one, please.You're in the way. There we go, like - okay, like that.Okay.And another Schnidt, please. So here's the -you can see the white. Yep.And a knife.And then the Hassan, please.Hold on.Okay, so we're no question about that -hold on a second.
I just want to make sure ofthat so we have no question we're going to go like this -right there and like this.That way we know... Is this a good line?Yeah, that's fine. Go ahead.Keep it pushed in - just so we don't lose that, okay.Hold on, make this - put it in as far as it will go in terms of getting somesecurity. Yeah - okay, and then you can take these.Can we get high flow on the CO2, please?
Gas is on. Thank you.Hold on.And then wrap it.
Yep, you'll see. Okay, take that, and then let's put the scope in.Can we have the room lights off, please?So then we're going to look up here.The liver looks good,nice and healthy, right? Yep.Can you look down at the liver for a minute -just one? Look down - yeah.And I think we need a little bit of focus. And I'll take thelocal anesthesia, please. Yeah, there we go.
Okay, watch that.Knife and a 12-mm trocar.So on the right side, I use a 12 trocar in the epigastric becauseI like to use the Endo Paddle,which works very well in retracting the liver.It's got a broad base, the felt is,you know, soft material - I'll take the Endo Paddle, please -that doesn't dig into the liver,but it does require a 12-mm trocar.On the left side, I just use thefan retractor on the spleen and pancreas topull that over. Okay, so what we're going to do is...Let's see.This is a little stuck there. We may have to...Take those down? It's possible.Usually, you don't have totake anything down in terms of the colon, butin this particular case, it might be a little stuck,we'll see - right there.Huh, interesting.You usually don't have to do that.She had a gallbladder in 1992.Yeah, okay. So, why don't you - let's put in the other trocars.Okay.So, let's see, go farther lateral on the first one just to sort of see where...This is where you had marked it. I know, but don't, yeah -Yeah, well don't go - yeah, but it doesn't matter where I marked it.Go out more lateral.Can you go out farther lateral? This is as far as - with this I can go more.You may want to do that out there - not that far out.A little bit closer in - like maybe just up - yeah, like there.Okay, try that. So, some local.Okay, good - and then we'll get another onesort of in between. That's - so this is why I like to go -do it from over there, you know? I mean, with a couple ofstands you can, you know, it works. Okay, yeah, we can try that.Well, I don't know, I like it that way, but...Where do you want this, here? Closer to us - closer,there I think, yeah.Okay. Good?Yep.So on the left side for an adrenalectomy,I always take down the splenicflexure of the colon.You sort of have to do that to get adequate exposure.On the right side, you almost never have to take down the colon at all.This is only because ofadhesions from the prior gallbladder surgery I guess.
Okay, go ahead.So there's a fair amountof tension on the tissue already, soyou can just pretty much go ahead and take these down.Mm hmm.Mm hmm, it's on a lot of tension so just - yep.Yeah, that's the gallbladder fossa, right? We don't -we don't really need it -okay, so let's go over here.
CHAPTER 4
So you already can see the -hold on a second. The adrenal -very easily. You see it? That's the adrenal, and here's the IVC.There's the kidney.Maybe a cyst on the kidney -is that what that is? In any case,can you hold the scope for a minute?
I'll open up this Endo Paddle,so it gives you - again, it gives youa nice, broad view - exposure, so -often - let's vent a little bit - often, I start by taking downthe lateral attachments of the liver.I think we should do that alittle bit because it's already pulling.I don't think we have to do toomuch here, but - in this particular case, butit'll just allow us to - so just pushdown and you can just get some of those attachments.So I bring the Endo Paddle and just sort of bring it up towardsme a little bit.This is the end of my... Yeah, yeah.You might be able to put the trocar in more.Okay, yep.Yeah, so let's get the suction/irrigation and just clean that outfor a second.
Let's continue where -where you were and just take down the peritonealattachments to the liver inferiorly. Careful.So you're going way up, so we can start out lateral and just -you want to be just a millimeter or two away from the liver, yep.Good.And just get in that groove and there you go - zip, zip.So we're going to lift the liver up and get to thesuperior aspect of the adrenal gland down to theretroperitoneal muscles, diaphragm.So with the other instrument, you shouldpush down on the adrenal gland, just carefully.Yep.And you want to almost bring the gland towards you by pulling -yeah, yeah, yeah, and I'm going to get thisretractor better, and then we just keep going until weget down to the muscle, down - lower, down - well, I mean,down - in other words...Closer to the adrenal?Yeah, just stay away from the liver a little bit - yep, okay.Mm hmm.You want to sort of head towards the back - posterior.Towards her back? Yeah.Her back, which is straight down. Yeah.I can't tell if that's a vessel.Yeah, careful, careful. That's - okay, that you can do, that's fine.So again - you got to - stop for a second - you have to pushdown on the gland - yep -so that we make sure to just pull it up.Because, I'm not - so that looks like a little accessory vein tothe cava, which you often see,so we're going to stay on our side of that. Okay.So you can get right in that groove, but I would go up right there.Yep - and just adjacent to that - exactly, right there.But use your other instrument to push down, so -and then the - you can usethe harmonic to - that's fine -you can use the harmonic to push a little bit toshow you the - show you where you are.Up - go up higher -so it's right...Here. Push away, yes.You want it to go in different directions:one down, one up. And then -and then grab it if you can. So, well, that's bleeding. Okay.So, let's go out here, lateral.Here?Out farther lateral - back, towards the back. Here?Yeah.And you got to go beyond the gland.The gland is right there. The gland's right here?Yeah, so you have to go beyond the gland. Right here?Yeah, and you want to pull the gland towards you.Yeah, that's it.And then go deep. Pull it - pull it and go deep.Here? Out lateral to find the muscle.I see. I see. See the muscle back there?Okay, that's what you want to do. Get beyond it -get beyond it,and pull it - pull it towards you.Yes! See how it comes off? Yep.It's the same thing on the left side, how we can -you can sort of sweep it off of theretroperitoneal muscle and diaphragm.Mary, could you bring the screen closer to me?So bring it down.Yep.And then keep coming - you got to keep coming down to - inferiorly, yeah.Okay, so now we can...You see the kidney here, right?Let's start making the - find the cleft betweenthe kidney and the adrenal, so...I'm going to score a little here. Yep.Okay? Mm hmm.Yeah.Right? Keep going out lateral - go out lateral.Here? Like here? Yeah.Yeah, chop through all that - yep.And again, you know, you haveto start making your way deep to the muscle.So not on top, you have to go down deep.Down more? Yeah, but you can getall that stuff all the way out to the - yeah.Okay, got it. Score all the peritoneum here. Yeah, yeah.So you have to kind of dig in there with both instruments -reverse chopstick -one goes one way, one goes the other - and then dig in.And dig.Go ahead, dig - you're just rubbing on top.You're not getting - so dig -dig into it with the instrument. Go ahead, get it.You're not, you're not - I mean, grab it - grab it with the -Grab it? No, with the -with your harmonic so you can get it.Oh, like actually - oh, like actually...Dig in, right, right.I thought you wanted me to bluntly dissect.Well, you can only go - I mean, if you can, but it's not -you're not making progress if it's sort of a...So you want to get deeper, yep.I see. Yeah.Can you vent, Connor? Thanks.So go in there. Dig in one way and then the other.Here? Yeah.More lateral still?Well just - that's fine. You're good, you're good, you're good.I just like to do reverse chopstick if that makes sense.Like this? Yeah, but down,deep, deep, deep, deep. Yeah. Yeah, it's the angles.Yeah, I know it is. Go ahead and now grab it.See, now you can grab all that stuff.Yeah.Yeah, keep pulling... I'm going to get the stuff in the foreground, I think that's...No, no, get - no, no, no - just keep going.You're going to get - your going to be good. You're going perfectly - yep.Before you know it, you're going to be down to the muscle. Okay.So, go ahead, just keepgoing deep.As long as you're going through that fat, you're in good shape.Okay.All right, so keep going lateral, yep.Sometimes I can help a little bit with this,and then go deeper - go deeper.I know, I know, I - you're going to getit, but I want you to... Like I've been saying all day,I trust you, Dr. Hodin.Go ahead, yep.See, muscle! I see it.See, once you get to the muscle,then it just - and then itjust comes right off. It's really simple. Yep.So I'm going to go and just kind of help you a little bit withthis, and then it just - yeah, you don't have to be out that far.I'm just going to... Okay, that's fine.Coagulate this. But, we're just...Yep.Yep, and then you can get behind thereand get some of those attachments underneath, yep.Do you see the liver?The liver's right here, you want me to get that?Just get it - it's just on a lot of tension, so we're just going torelieve that a little bit.Okay, and then that gives us a better view of -you know - careful, we don't want to get the diaphragm.Yep. Good.All right. Okay, so now,if we go back to this, you can - can you justget the adrenal back down, yep.Okay, so now, I'm going to straighten things out a little bit.Yeah, don't grab.We're going to want to get between the cava and theadrenal, okay?
CHAPTER 5
So,I'm going to go in carefully.So here's cava.Here's the adrenal gland - there, you can see there's a tumor right there, right?It's bulging out a little bit. So we do have to get the peritoneum.Once you make an opening...Just one second, I want to just get in there.So I feel like we're a little -can I get the clip applier, please?You mean the 5-mm one, or do you want...Yeah, 5-mm clip applier.That shouldn't be anything there really, but...You can see...It's a little over it, like, you can see the cava right under you.Yeah, so my point is here, well -are we straight? I feel like we're not straight.So you can go in with both instruments,and you push the cava one way.And I go deeper with the suction and go the other way, and if you keep going,you're going to - yep,see, I'm going one way, I'm making it a little tunnel, but...And I'm pushing down to the muscle. So this is all just -extra adrenal - periadrenal fat,and it's going to get us down tothe muscle -eventually.Aren't you nervous about touching the cava with the hot instrument?Or not really?Not really. I know people worry about that a lot,and I've never - so there's muscle. Yep.Actually, this could be the adrenal vein right there, right? Yeah.Because this is all -so this is actually - this is probably the adrenal vein that's -we're not seeing it so perfectly, but...Oh, maybe not - no, maybe not, maybe not.This looks like it, here.Yeah, maybe it's just -and there's more adrenal up there. So, I'm going tojust go like this for a minute.See the adrenal tissue under there?So again, I mean, I - you don't have to do this all now,but I'm just doing it to make the point: how easy it is to getthis because if you go out here, look. This is going to be veryeasy to take the rest of that. Yep.I'm going to just put a...Clip on that?Clip on just because -sort of in case.So it loads.Can I have the harmonic back? Do you think that's the vein?I don't, honestly.I guess we'll find out.Didn't seem very - like there's much of a structure to it.So you see how this just...Yep.It's all incredibly safe. Yep.You can lift it up. Yep.You can't hurt anything. Right.We're going to be able to get all that. Now...That's our vein there, I believe.Now the vein - so there's adrenal.The vein's going to be in here,right? Oh, there - there it is - right there. Yeah.So again, I think we're not entirely...Let's get more - pull up on liver. Yeah, there you go.
So therewe can see the vein more clearly.Adrenal vein's very easy to get once -once you see it, it's just -there's always a space there that's easy todelineate so you can just sort ofgo like that.I'm just making it a little more clear, but we could clip at anytime.So it just lifts off the retroperitoneum so easily.Okay, so...And this all - again, it's all just...Okay, you want to come and take the vein?Sure, or you can do it. It's fine.You don't care? No.Okay, I'll take clips.5 mm is okay?Yeah, I do it just because we have the 5-mm trocar.So, we'll make sure one nice one on thevena cava, another one -on the cava side.Uh, let's see. I should have gone up higher.Okay, that was not - yeah.Scissors, please. Oh, that was notexactly what I was planning.That's why you should have done that.Let's see. Let's make sure that we're...Yeah, below your clip, on the vena cava side,it's like - was oozingwhen there was tension on it, so...Yeah, it's fine. Harmonic, please.It's basically done.So we just get theremainder of the attachments.We still have to take it away from the livera little bit but let me just -So now let's see where -where it's meeting the liv - the kidney right here.Mm, yeah, there's a big vessel there though.Shouldn't be. Where?It just keeps pulsating right under there.Where do you mean? Here? Yeah.Well that's going to be the renal artery. Yeah, I'm just saying...Yeah, so we're going to stay away from therenal artery, so I'm going to push theadrenal sort of up and away, so we make sure to stay away fromthe hilar vessels.So I'm kind of getting under and trying topush it away.Can you clean that for me, please?So let's see what we've got here. You've got -that's -where you're going to take it off the kidney, huh?There you go.Yep, and actually out this lateral, you know... Here?Yeah - you really can't hurt anything,you know, once you're beyond where the renal vessels are going to go in.I mean, there can be a superior branch that's -you can see it under there - but like you said pulsating, but...Yeah.And do you still like to use this instrument for this?Well, to keep the - at some point,you can just grab, you know? Right, exactly.When you sort have enough, but go ahead, you're right there.Yeah, you see the kidney? The kidney is right here.Yeah, is that - what is - wait, what is that right there?What is that? It's just a...A vein, but I think that's...How is that possible?Yeah, I think it's just. Yeah. It's just a fold? It's just a fold of - okay.Go ahead. Yeah, it should just be - there shouldn't beanything, so - but go ahead, let's go. Okay. Because my...Get close to the - yeah, get close to the adrenal. The adrenal's up here.Underneath there, yeah. Uh huh.Mm hmm, just lift it up, yep.Can I switch this for a grasper? A grasper, yeah.Just suction out once. While you're there,just suction it out, just to clean it a little bit.So grab down here. If you grab - grab down - no, grab right there.Yeah, like this, just come here, come right up, yeah.And then I'm just going to go here. Go chop, chop - yep.Mm hmm.Can we have an Endo Catch bag?Okay, grab it. That's it. Is that it?Yep.Let's see. Suction/irrigation.Let's just - can you pull - pull it -make sure it's all completely detached. Is it? It definitely is, yeah.Yeah, okay.
So we'll just -this looks good. There's the cava. There's our two clips.Mm hmm, just suction out that little - yep.Do you want me to irrigate?Sure, go ahead.Yep, that's fine.Looks good.All right, so I'm going to let the liver fall down. Okay.
CHAPTER 6
And if you can hold the scope for just a minute. Mm hmm.I'm going to take this Endo Paddle out.I love these cases.And then we're going to take the scope,put it into the epigastric site,and we'll take the Endo Catch bag.So...And drop it in the bag. Yep, that's fine.And then, if you could just close it up.Here, I can hold the camera. Okay.Okay so - Kelly, please.Scissors.There's that.Let's just take those other trocars out under direct vision.That looks fine. This looks fine.Okay, so we're going to take this.And room lights on, please.All right, so we'll go like this.And then we'll see. Oh, okay.Can I get a sponge and a scissors?
CHAPTER 7
So we're going - I'm going to take a look at the lesion.Can I get a knife, please? So,this is an aldosteronoma, we believe, so weexpect it to be a cortical lesion.And that's what it is, clearly - can I have another - actually, I'll just -clearly, that's a nice, yellow, lipid-rich cortical adenoma.So, it's -it was supposed to be 2.5 cm, right? That's -about correct, and then let's just see here.The adjacent, normal adrenal will be out here.You can see that little, thin... Oh yeah.Can you see it there?Oh, that's so cool.You can see the -cortex and then the line -dark line in the middle of the medulla.So this is a nice cortical lesion.Okay, so we'll put this in the pathology cup. Okay, that'sright adrenal gland, and let's see -can I have a wet and a dry, please?And two narrow Richardsons and a 0 Vicryl. We'll close up the fascia.
CHAPTER 8
All right, let's put a stitch above, below, and then we'll tie these together.Mm hmm.So we will watch her in the recovery room for probably 3 or 4hours, and if she's okay, she can go home today. Otherwise,if there's any question,we can keep her overnight,but it's pretty safe to send these patients home.Pull it through. Oh, wait, I'm not. Oh, okay.Just so we don't... Okay, I just wanted to go across.Uh huh.Can I get a sponge, please?So, that's the apex, right?Mm hmm.Did that get both sides? Sort of did, huh?Yeah. Yeah, I think so.We'll get...Let's see here. So then we'll go like this.I'm going to come through the middle.Mm hmm.I like how it was so short. I know.I've done them - I mean,honestly, if - I've done this operation in 20 minutes.It's not always 20 minutes, but you can see how easy it can be, I mean…
CHAPTER 9
So we just completed the laparoscopic right adrenalectomy.Everything went fine -it was a pretty straightforward case.We saw the lesion in the adrenal gland even laparoscopically, andthen once the specimen was out, sort ofconfirmed that this wasas expected - about a 2.5-cm cortical adenoma.No real surprisesfrom the standpoint of the dissection or the anatomy,and she did well throughout the case.Usually, I send these patients home,assuming they don't have significant medical comorbidities.The incisions,the port sites, are essentially the same as we do forlaparoscopic cholecystectomy, whichof course is done routinely as an outpatient, so as longas there aren't significant eithercomorbid conditions or sort of an endocrine reasonfrom the standpoint of the adrenal tumor to keep the patient inthe hospital,I do tend to send most of these patients home the same day andkeep track of themclosely with telephone calls tonight and tomorrow.And the patient was anxious to go home,so we'll see if that works out.Of course, she's going to take her blood pressure at home.I usually have patients take ittwice a day and record so that I can see the levels but alsoher primary care,or whatever medical doctor's taking care ofher blood pressure meds.We'll send her out on reduced medications,maintaining the beta blocker for now.And we'll see what happens in the long runwith her blood pressure and her potassium. We'rehopeful based on the adrenal vein sampling thatthis is going to cure her hyperaldosteronism, and ideally,she'll be able to come off all of her blood pressure medsand certainly the potassium supplements, butonly time will tell whether there's any element of essentialhypertension and whether she'll need anyblood pressure meds at all, but we're hopeful atthis point, and we will see how it turns out.