
Open Distal Gastrectomy
Main Text
Table of Contents
A complete margin-negative (R0) resection remains the only potentially curative treatment for gastric adenocarcinoma. The choice of operation depends on the location of the tumor as well as the stage of disease. This patient presented with symptomatic anemia, and workup demonstrated gastritis and a small tumor in the distal stomach. Biopsies confirmed adenocarcinoma, and an endoscopic ultrasound (EUS) staged this tumor as T2 N0. Staging scans showed no evidence of distant metastatic disease. Given that this patient had a relatively early stage tumor, we elected to proceed with upfront surgery, which in this case entailed a distal gastrectomy. This video shows an experienced gastric surgeon’s technique for performing an open distal gastrectomy with an “extended” D1 lymph node dissection.
Although the incidence of gastric cancer in the United States has dramatically decreased during the past several decades, gastric cancer remains an important cause of cancer-related death. Despite significant improvements in staging modalities, surgical therapy, and perioperative care, the prognosis of most patients with gastric cancer remains poor. This is largely a result of the aggressive biology of this cancer as well as the advanced stage of disease at which most patients present to the clinician. Risk factors include Helicobacter pylori and Epstein-Barr virus (EBV) infection, pernicious anemia, prior gastric resection, smoking, and high salt intake. Approximately 10% of gastric cancers are due to inherited cancer syndromes, including hereditary diffuse gastric cancer (HDGC), characterized by germline mutations in the E-cadherin (CDH1) gene, and hereditary nonpolyposis colorectal cancer (HNPCC) syndrome, characterized by germline mutations in DNA mismatch repair genes. Recently, a comprehensive molecular evaluation of gastric cancer has led to a classification scheme that defines 4 major genomic subtypes and their approximate frequencies: EBV-infected tumors (9%), microsatellite unstable (MSI-high) tumors (22%), genomically stable tumors (20%), and chromosomally unstable tumors (50%).1
There are few, if any, classic symptoms suggestive of a diagnosis of stomach cancer, which explains why this cancer is frequently diagnosed at an advanced stage. Early symptoms, such as epigastric pain, dyspepsia, and acid reflux, are so nonspecific that most patients are simply treated empirically with antacids without further investigation. As the disease progresses, the symptoms become more prominent and more ominous and include such complaints as dysphagia, nausea, vomiting, early satiety, anorexia, fatigue, and weight loss. The location and histologic type of gastric cancer often dictates the symptom complex, from dysphagia for proximal tumors to vomiting for obstructing distal tumors to early satiety and weight loss for diffuse-type (linitis plastica) tumors.2,3
This patient is an 84-year-old gentleman with a history of gastritis and a chronic gastroesophageal junction stricture who presented to his primary care physician with symptoms of fatigue and shortness of breath. A complete blood count was obtained and showed that the patient was anemic. He denied abdominal pain, nausea, vomiting, change in bowel habits, difficulty eating, or weight loss.
The physical examination of a patient with gastric cancer is typically unremarkable with perhaps the exception of epigastric abdominal tenderness and, less likely, of a palpable epigastric mass. Classic eponymous physical findings such as Virchow’s node, Sister Mary Joseph’s periumbilical node, and Blumer’s shelf are rarely present but when seen indicate advanced metastatic disease. Similarly, the presence of cachexia, jaundice, ascites, and hepatomegaly in a gastric cancer patient typically signifies incurable metastatic disease. Our patient was well-appearing, and on examination he had a soft abdomen and no palpable masses.
 Figure 1. Upper endoscopy showing mass in prepyloric region of stomach for the patient in the video.
Figure 1. Upper endoscopy showing mass in prepyloric region of stomach for the patient in the video.Imaging for workup of gastric cancer includes a variety of studies. The diagnosis of gastric cancer is usually readily established by endoscopy with biopsy (Fig. 1). Endoscopy defines the location and extent of the tumor within the stomach and, when combined with endoscopic ultrasound (EUS), allows for accurate estimation of the depth of tumor invasion (T stage). EUS is the most sensitive modality in establishing the T stage of a gastric cancer, and EUS enables an assessment of the regional lymph nodes and needle biopsy of suspicious nodes to confirm nodal involvement (N stage). A CT scan of the chest, abdomen, and pelvis should be performed to evaluate for distant metastatic spread, such as to the lungs, liver, peritoneum, or lymph nodes outside the field of resection. In addition, a CT scan is sensitive in detecting even small amounts of ascites that may represent peritoneal tumor spread and that can be sampled by image-guided means for cytologic examination. Though PET and PET–CT scans are not routinely recommended in the preoperative staging of gastric cancer, they may certainly provide additional useful information. PET has a low sensitivity in detecting the primary tumor, especially in early and diffuse-type gastric cancers, but PET has a higher specificity than CT (˜90% vs. ˜60%) in the detection of regional lymph node metastases and has a reasonable sensitivity for the detection of liver, lung, and distant lymph node metastases.4 In addition, PET can be used to monitor tumor response to neoadjuvant chemotherapy, as it accurately detects responders to therapy at an early stage, thus enabling the clinician to maintain patients on as active a chemotherapy regimen as possible.
Patients with locoregionally advanced cancers (T3+/N+) are considered for additional staging by laparoscopy. Staging laparoscopy can be done immediately prior to the planned laparotomy or as a pretreatment procedure performed in patients considering preoperative therapy. Staging laparoscopy upstages more than 30% of patients through the identification of radiographically occult peritoneal and liver metastases and positive cytology.5
Gastric cancer typically spreads via the lymph nodes or hematogenously and commonly metastasizes to the liver, lungs, or peritoneum. It can also spread directly to involve adjacent organs, such as the pancreas and transverse colon. The only potential curative therapy for gastric cancer is surgery. Even with complete, margin-negative resection and (neo)adjuvant therapy, the 5-year survival rate remains low at ~40%.
The most common treatment paradigm for gastric cancer in the United States has historically been upfront surgery, followed by adjuvant chemoradiation therapy (as described in the Intergroup 0116 trial) for those patients with high-risk (T3/4, node positive, poorly cohesive-type) tumors.6 However, only 64% of the patients in this trial could receive the postoperative chemoradiotherapy as planned, and so many favor perioperative chemotherapy for such patients, as described in the MAGIC trial conducted by the British Medical Research Council. In this trial, patients were randomized to receive either perioperative chemotherapy (three cycles of Epirubicin, Cisplatin, and 5-fluorouracil (ECF) preoperatively and postoperatively) and surgery or surgery alone. Five-year survival rates were superior in the perioperative chemotherapy group compared with the surgery-alone group (36% vs. 23%).7 Though only ~ 40% of patients complete all of the recommended therapy with this treatment approach, more than 85% of patients receive all 3 planned cycles of preoperative chemotherapy, and all patients receive at least one cycle of chemotherapy. Administration of at least a few cycles of systemic therapy in advance of surgery for patients with high-risk tumors confers several advantages: (1) it permits early treatment of possible micrometastatic disease; (2) one can monitor the in vivo tumor response to the therapy, such as with PET–CT scan imaging; and (3) one can select for those patients with particularly bad tumor biology who develop early metastatic disease and who would thus derive no survival benefit from gastrectomy.7
A complete margin-negative (R0) resection remains the only potentially curative treatment for gastric adenocarcinoma. The choice of operation depends on the location of the tumor as well as the stage of disease. Superficially invasive (T1a) gastric cancers of favorable histologic grade can be treated by endoscopic mucosal resection or wedge excision with or without concomitant sentinel lymph node biopsy. Such procedures have been extensively described by our surgical colleagues from Japan, where gastric cancers are frequently diagnosed at an early stage given the prevalence of screening endoscopic examinations in that country. Because the majority of patients in the United States present with symptomatic, locoregionally advanced tumors, the primary surgical question is which procedure offers the greatest chance for cure with acceptable morbidity and mortality. Many patients are not candidates for any surgical procedure either because they are medically unfit or because of the presence of metastatic disease seen on preoperative imaging studies or at the time of laparoscopy. For those patients who are candidates for gastric resection, the options include total, proximal, and distal gastrectomy. There is an increasing worldwide experience in performing these procedures laparoscopically, with improved short-term outcomes and nodal yields, and survival outcomes that are on par with the traditional open procedures. However, the vast majority of resections for gastric cancer in the United States are still performed via the open approach.
Patients who should be considered for immediate surgical resection include those with early stage (T1/T2 N0) gastric cancers and those who require immediate palliation of bleeding or high-grade tumor-associated luminal obstruction. However, the perioperative morbidity and mortality rates in this latter population of patients are significant and must be carefully weighed against the likely benefits of resection. Patients with locoregionally advanced gastric cancers are good candidates for preoperative chemotherapy or chemoradiation therapy.
Because this patient had a relatively early stage tumor (uT2N0) and was in remarkably good health for his age, he was offered upfront surgery with a distal gastrectomy. We felt that an open distal gastrectomy limited the risk of overtreatment with neoadjuvant chemotherapy for a potentially low-risk cancer, while leaving us the option to offer him adjuvant therapy if the final pathology report revealed a more advanced (eg, T3+/N+) cancer.
The extent of gastric resection is determined by the location and extent of the primary tumor. Prospective, randomized trials failed to demonstrate a survival advantage for total gastrectomy over distal, subtotal gastrectomy for patients with tumors of the distal stomach.8 Therefore, for those patients in whom a 5- to 6-cm margin from the tumor can be obtained while still maintaining a reasonably-sized gastric remnant, a more conservative gastric resection should be performed, as this confers an equivalent survival rate with less morbidity and a better quality of life than does a total gastrectomy.8 Nonetheless, a total gastrectomy should be performed if necessary to achieve an R0 resection, as positive resection margins (R1 resections) lead to very poor survival. In the Dutch gastric cancer trial, 10% of patients had a positive resection margin and a correspondingly inferior 3-year survival (18% vs 63%) compared with those who had a negative resection margin.9 However, microscopically involved margins appear to affect long-term survival only in those patients with five or fewer lymph node metastases. For proximal gastric cancers, many surgeons prefer a total gastrectomy over a proximal gastrectomy owing to the long-term sequelae of symptomatic acid reflux with the latter procedure.
The extent of lymph node dissection is one of the most controversial issues in the management of gastric cancer. Reports from the Gastric Cancer Registry and other retrospective studies have made radical gastrectomy with extended (D2) lymphadenectomy the standard of care for the treatment of curable gastric cancer in Japan.10,11 The Japanese Research Society for Gastric Cancer categorizes the draining lymph node basins of the stomach into 16 stations, including 6 perigastric stations (Figure 2a) and 10 regional stations along the major vessels and adjacent to the pancreas (Figure 2b). The extent of lymph node dissection is indicated by the designation D. A D1 dissection includes only the perigastric nodes (stations 1 to 6); a D2 dissection includes the lymph nodes along the common hepatic, left gastric, celiac, and splenic arteries (stations 7 to 11); and a D3 dissection includes additional nodes within the porta hepatis and adjacent to the aorta (stations 12 to 16) (Figure 3).
 Figure 2a. Lymph node stations including the perigastric, or D1, lymph nodes (stations 1 to 6).
Figure 2a. Lymph node stations including the perigastric, or D1, lymph nodes (stations 1 to 6).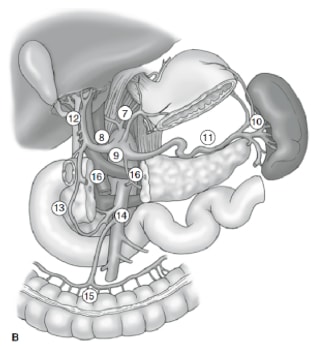 Figure 2b. Lymph node stations including the regional, or D2 and D3, lymph nodes (stations 7 to 16).
Figure 2b. Lymph node stations including the regional, or D2 and D3, lymph nodes (stations 7 to 16).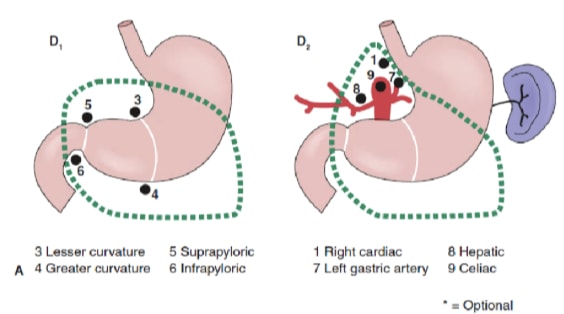 Figure 3a. Extent of gastric and lymph node resection for lower one-third lesions.
Figure 3a. Extent of gastric and lymph node resection for lower one-third lesions.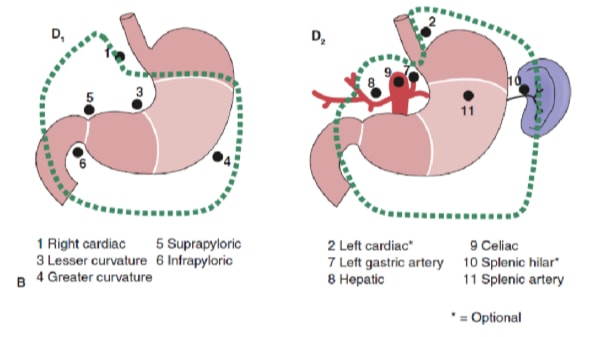 Figure 3b. Extent of gastric and lymph node resection for middle one-third lesions.
Figure 3b. Extent of gastric and lymph node resection for middle one-third lesions.Two large, prospective randomized trials comparing the outcomes of D1 dissection with those of D2 dissection have been conducted in Western patients. Fifteen-year follow-up of the larger of these two studies, namely, the Dutch Gastric Cancer Group Trial, demonstrated no long-term overall survival benefit with the D2 lymph node dissection (29%% vs 21%, P = .34) but did show a significantly decreased gastric cancer-related death rate (37% vs 48%, P = .01) and a lower locoregional recurrence rate than D1 surgery.9 However, there were significantly higher rates of postoperative morbidity (43% vs 25%) and mortality (10% vs 4%) in those patients undergoing the more extensive D2 lymphadenectomy, in large part resulting from the greater numbers of splenectomy and pancreatectomy performed in this group in order to achieve a complete node dissection.9 Similarly, the British Cooperative trial conducted by the Medical Research Council reported an increased morbidity, associated with high rates of concomitant splenectomy and pancreatectomy, without a benefit in overall or recurrence-free survival in those patients randomized to a D2 dissection.12
Despite the findings of these two studies, investigators have argued that if the complication rate after an extended D2 lymph node dissection could be decreased, the survival benefit conferred by a D2 dissection, as reported by experienced centers in Asia, might be translated to Western patients with gastric cancer.13 Thus, the Italian Gastric Cancer Study Group conducted a phase III trial randomizing patients to either a pancreas-preserving D2 lymphadenectomy or a D1 lymphadenectomy at high-volume centers by surgeons who completed rigorous training in the technique through observation of master surgeons in Japan. They reported impressively low morbidity (17.9%) and mortality (3.0%) rates in patients undergoing the D2 dissection, in which a pancreatectomy or splenectomy was performed only for direct tumor invasion.14 However, they found no difference in 5-year overall survival between the D1 and D2 groups (66.5% vs 64.2%; P = 0.695), though subgroup analyses suggested that a D2 lymphadenectomy may be of benefit to patients with T2–T4 and/or node-positive tumors.14
It remains unclear whether a D2 lymph node dissection is simply a thorough staging procedure or whether there may be a therapeutic benefit for certain subsets of patients (eg, patients with N2 disease). It should be noted that the accurate staging of patients with gastric cancer, according to the most recent seventh edition of the American Joint Committee on Cancer (AJCC) Staging Manual, demands the evaluation of at least 15 lymph nodes.15 The nodal staging is then based on the number of positive nodes with N1 (1 to 2 positive nodes), N2 (3 to 6 positive nodes), N3a (7 to 15 positive nodes), and N3b (16+ positive nodes) categories. Studies have shown a correlation between improved patient survival and larger numbers of lymph nodes examined in the specimen.16 Of course, this may simply reflect more accurate staging as opposed to a therapeutic benefit from the procedure. However, there is indirect evidence that more extensive lymphadenectomies result in lower rates of locoregional recurrence, and this may translate into a survival benefit. Indeed, a randomized trial conducted at a single center in Taiwan identified an overall 5-year survival advantage for those patients undergoing a D3 dissection (59.5%) compared with those undergoing a D1 dissection (53.6%).13
For patients treated at MGH over the past decade, we have reported morbidity and mortality rates after gastrectomy and D2 lymphadenectomy of 17% and 0%, respectively, and our median lymph node yield with ex vivo dissection of the specimen has increased to 40 nodes. The median length of stay for subtotal and total gastrectomy in the United States averages 9–10 days, though many patients are discharged within 7 days. The long-term complications of subtotal and total gastrectomy include vitamin and mineral deficiencies, particularly of vitamin B12, vitamin D, iron, and calcium, and the classic postgastrectomy syndromes, such as alkaline reflux gastritis, dumping syndrome, Roux stasis syndrome, and afferent limb syndrome.
Surgery is the only potentially curative therapy for localized gastric cancer, yet even for those patients in whom an R0 resection is possible, only 35% to 40% 5-year survival is achieved with either perioperative chemotherapy or postoperative chemoradiotherapy. Future progress in the treatment of gastric cancer depends on the development of better systemic therapies as well as techniques for earlier diagnosis.
A. DISTAL STOMACH RESECTION:
Gastric adenocarcinoma, tubular type, mismatch repair protein expression instable. (See synoptic report).
B. LYMPH NODE BIOPSY, STATION 8:
There is no evidence of malignancy in four lymph nodes (0/4).
C. LYMPH NODE BIOPSY, STATION 11:
There is no evidence of malignancy in two lymph nodes (0/2).
D. LYMPH NODE BIOPSY, STATION 7:
There is no evidence of malignancy in two lymph nodes (0/2).
E. LYMPH NODE BIOPSY, STATION 3:
There is no evidence of malignancy in one lymph node (0/1).
SYNOPTIC REPORT:
TUMOR STAGE SUMMARY: pT1bN0.
SPECIFIC SITE: Gastric antrum.
TUMOR SIZE (Greatest dimension): 0.3 cm (as measured on slide).
WHO CLASSIFICATION: Tubular adenocarcinoma.
HISTOLOGIC GRADE: G1 (Well differentiated)
EXTENT OF INVASION: pT1b (Tumor invades submucosa).
SMALL VESSEL (BLOOD/LYMPHATIC) INVASION: Absent.
LARGE VESSEL (VENOUS) INVASION: Absent.
PERINEURAL INVASION: Absent.
PROXIMAL GASTRIC MARGIN: Uninvolved by invasive carcinoma.
DISTAL DUODENAL MARGIN: Uninvolved by invasive carcinoma. (clearance= 0.4 cm).
REGIONAL LYMPH NODES: pN0 (No regional lymph node metastasis): 31 lymph nodes examined.
*The lymph node total is inclusive of all specimen parts. The main specimen (specimen A) contained 22 lymph nodes.
HER2 IMMUNOHISTOCHEMISTRY: Her 2 score 0/negative (No reactivity or very faint membranous staining in < 10% of tumor cells).
Additional Studies:
MLH1 and PMS lost.
MSH2 and MSH6 intact.
Additional findings:
Gastric antral mucosa with intestinal metaplasia and high grade dysplasia.
Fundic gland polyp.
Epstein-Barr virus encoded RNA (EBER) is negative.
Our patient recovered well from surgery and was discharged on postoperative day 5. His final pathology report staged his tumor as T1bN0, and the margins of resection were negative. We achieved an excellent nodal harvest (31 lymph nodes), so we can be confident in the accuracy of this stage assignment. As such, he does not require adjuvant therapy, and his long-term prognosis is excellent.
A fixed abdominal wall retractor system can be very helpful for this operation; we used the Bookwalter, but other options include the Thompson and Omni retractor systems. The duodenum and stomach are transected with staplers—in this case an Endo-GIA stapler. A vessel sealing device, such as a LigaSure device or Harmonic scalpel, are quite helpful in the efficient control of small blood vessels. Larger vessels, such as the left gastric artery, can be divided with a vascular stapler or controlled by traditional suture ligation.
The authors have no conflicts to disclose.
The patient referred to in this video article has given his informed consent to be filmed and is aware that his personal health information will be published online in unidentified fashion.
Citations
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature. 2014;513(7517):202-209. doi:10.1038/nature13480.
- Mullen JT. Gastric cancer. In: Fischer J, ed. Mastery of Surgery. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2017.
- Yoon SS, Park DJ. Gastric adenocarcinoma. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 11th ed. Philadelphia, PA: Saunders, 2014:87-95.
- Yun M. Imaging of gastric cancer metabolism using 18 F-FDG PET/CT. J Gastric Cancer. 2014;14(1):1-6. doi:10.5230/jgc.2014.14.1.1.
- Ikoma N, Blum M, Chiang YJ, et al. Yield of staging laparoscopy and lavage cytology for radiologically occult peritoneal carcinomatosis of gastric cancer. Ann Surg Oncol. 2016;23(13):4332-4337. doi:10.1245/s10434-016-5409-7.
- Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345(10):725-730. doi:10.1056/NEJMoa010187.
- Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11-20. doi:10.1056/NEJMoa055531.
- Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Gennari L; Italian Gastrointestinal Tumor Study Group. Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Ann Surg. 1999;230(2):170-178. doi:10.1097/00000658-199908000-00006.
- Bonenkamp JJ, Hermans J, Sasako M, et al; Dutch Gastric Cancer Group. Extended lymph-node dissection for gastric cancer. N Engl J Med. 1999;340(12):908-914. doi:10.1056/NEJM199903253401202.
- Maruyama K, Okabayashi K, Kinoshita T. Progress in gastric surgery in Japan and its limits of radicality. World J Surg. 1987;11(4):418-425. doi:10.1007/BF01655804.
- Sasako M, McCulloch P, Kinoshita T, Maruyama K. New method to evaluate the therapeutic value of lymph node dissection for gastric cancer. Br J Surg. 1995;82(3):346-351. doi:10.1002/bjs.1800820321.
- Cuschieri A, Weeden S, Fielding J, et al; Surgical Co-operative Group. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Br J Cancer. 1999;79(9-10):1522-1530. doi:10.1038/sj.bjc.6690243..
- Wu CW, Hsiung CA, Lo SS, et al. Nodal dissection for patients with gastric cancer: a randomised control trial. Lancet Oncol. 2006;7(4):309-315. doi:10.1016/S1470-2045(06)70623-4.
- Degiuli M, Sasako M, Ponti A; Italian Gastric Cancer Study Group. Morbidity and mortality in the Italian Gastric Cancer Study Group randomized clinical trial of D1 versus D2 resection for gastric cancer. Br J Surg. 2010;97(5):643-649. doi:10.1002/bjs.6936.
- Edge SB, Byrd DR, Compton CC, Fritz AG, Greene F, Trotti A, eds. AJCC Cancer Staging Handbook. 7th ed. New York, NY: Springer; 2010.
- Smith DD, Schwarz RR, Schwarz RE. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: data from a large US-population database. J Clin Oncol. 2005;23(28):7114-7124. doi:10.1200/JCO.2005.14.621.
Cite this article
Andrea L. Merrill, MD, John T. Mullen, MD. Open distal gastrectomy. J Med Insight. 2024;2024(191). https://doi.org/10.24296/jomi/191Procedure Outline
1. Patient is positioned supine on operating table.
2. Anesthesia and antibiotic administration (usually a cephalosporin).
3. Upper midline incision (xiphoid process to below umbilicus).
4. Division of falciform ligament.
5. Abdominal exploration (for extent of locoregional disease and distant metastases).
Special attention: peritoneal surfaces and liver.
- Evaluation of remote lymph nodes for metastases.
6. Mobilization of the greater curvature with omentectomy and division of the left gastroepiploic artery.
7. Infrapyloric mobilization with ligation of the right gastroepiploic artery and vein as it enters the gastrocolic trunk.
8. Superpyloric mobilization with ligation of the right gastric artery.
9. Duodenal transection.
10. Lymphadenectomy with dissection of the porta hepatis, common hepatic artery, left gastric artery, celiac axis, and splenic artery, and ligation of left gastric artery.
11. Gastric transection.
12. Reconstruction by Billroth II or loop of Roux-en-Y gastrojejunostomy.
Transcription
CHAPTER 1
Hi I'm Dr. Mullen. I'm a surgical oncologist at the Massachusetts General Hospital. I specialize in the treatment of gastric cancers and today we're going to operate on an 80-ish-year-old gentleman who has a distal gastric cancer. He initially presented with anemia, which led to an upper endoscopy. The endoscopist noted an area of inflammation in the distal stomach. That then prompted some biopsies which showed very early intramucosal adenocarcinoma. Patient was then referred for an endoscopic ultrasound, which showed a more obvious tumor invading the muscle of the stomach, and so we staged as T2. There were no suspicious lymph nodes, and so the regional lymph nodes were staged as N0. Scan showed no signs of metastatic disease so he presents today for a potentially curative distal gastrectomy. In this procedure, we're going to remove the distal 2/3rds of the stomach. We'll also a dissect out the D1 lymph nodes adjacent to the stomach. But furthermore, we’ll take out what I refer to as the D1 plus lymph node. So those nodes in the D2 station immediately in the central arterial system So celiac axis, common hepatic artery, and proximal splenic artery. And then we'll probably reconstruct him with a loop gastrojejunostomy in a Billroth II fashion.
CHAPTER 2
So, clearly we're making an upper midline incision. The important thing here is to try to stay on the midline and not expose the rectus muscle on either side. We are doing a nice job here of staying in the midline. The fat here is the preperitoneal fat. When you do forget surgery, I do think it's important to carry your incision all the way up to the xiphoid and at times will come around the xiphoid as we are in this case. So the xiphoid is right here. He has a very prominent xiphoid. We're just going to come around that a little bit just to give us better exposure in the upper abdomen. Okay, DeBakey forceps.
Now when one enters the peritoneal cavity, you have a choice to do so either bluntly or sharply. We're going to do so sharply here that - that is through the preperitoneal fat. Now this is the peritoneum, which has much greater tentsile strength. Make it slightly larger so one can put your finger in and then use the cautery to open up the remainder of the peritoneum. Can I have my headlight on - is it Kathy - who's here? Kelly. There are often times small vessels in the preperitoneal fat, so it's worthwhile to take the time just to cauterize those as you go, so that you don't have bleeding into your field during the case. Great.
So the first step is to do an exploration of the abdominal cavity to make sure there's no sign of metastatic disease. If gastric cancer is going to metastasize, it most commonly does so to the liver or to the peritoneal surfaces. So we're examining the surface of the liver. If a patient has a more advanced cancer such as a T3 or T4 cancer or a node positive cancer or has a very high-risk histology like a poorly cohesive type cancer or a linitis plastica, then I will commonly do a diagnostic laparoscopy at a separate operative sitting, but since he had a T2 and N0 cancer the risk of metastatic spread is very low, so I usually do not do a staging laparoscopy and indeed there's no sign of metastatic disease on exploration here. What's this little thing? That's a diverticulum. Oh, okay.
CHAPTER 3
Great, so our first step is to take the omentum off of the colon. Oftentimes patients will have adhesions of the omentum as he does. We'll take that abdominal wall retractor. Okay. These can be a nuisance because often times these adhesions can be deep in the pelvis. For smaller cases like this, I find a Bookwalter retractor to be perfectly fine. It's a small incision - and yes Yeah give us one second cuz I think the wound protector will be tricky with this. Once we take the omentum down, then we'll put that in. Is that okay? Let's come across this way. Okay. Mhmm. I know it's hard to see. He's probably had a bout of diverticulitis in the past and his omentum did its job by coming down here to seal the perf or inflammatory process. Maybe right up here - yep. Maybe right there - can you see that? Yeah Great. It's important to take the omentum out in a patient with gastric cancer - DeBakey forceps - because we're going to devascularize it in this case, as we ligate both the right and left gastroepiploic arteries which are the source of blood supply. Furthermore, the station four lymph nodes live along the greater curvature in the omentum, and so for an adequate lymph node harvest we want to take out the entire omentum. Okay, great, we're all set, Lauren. So now we have our omentum into the field. This is another common sight of metastasis. This is a nice glistening normal omentum. There's no sign of metastatic disease here.
So step one of the operation, besides getting into the abdominal cavity, is to now enter the lesser sac through the gastrocolic omentum here. One trick I've found that's helpful is if you grab the stomach together with the omentum, that helps you get into the proper space and not come through the omentum. So now Andrea is going to enter this avascular plane between the transverse mesocolon and the back wall of the stomach. And here we can see the posterior wall of the stomach. This is the lesser sac. Now here we want to stay right in that avascular plane. If you’re little too far to the colon, you can get into either the mesocolon or these small appendices epiploicae and if you're a little too far this way, then you can get into the back wall of the stomach. In some patients, this procedure can be tricky, particularly if there's not a clear delineation between the two - the mesocolon and the back wall of the stomach. Thin patients, it can sometimes be tricky. In him, it's relatively straightforward. Small vessels can just be cauterized I prefer the LigaSure. Yeah, so you see now that's a nice plane there. You're going to want to... I'm just gonna fan it out. Yes. That vessel's going to go with the omentum. That's right. We’re carrying our dissection rightward now toward the mid-transverse colon, hepatic flexure. I do as much of this as I can without the retractor and then soon we're going to get to a point where it's going to become too deep and we'll have to put in our Bookwalter to complete the last bits of the dissection. The omentum can bleed throughout the case, and it becomes a bit of a nuisance, so I do like to control any little bleeders. So here's the appendices stuck to omentum. Now we should place the ring and the retractor as were getting a little bit deeper. The wound protector's designed to decrease your risk of superficial site infections.
One needs to be mindful of the falciform ligament here as one does not want to tear the liver so I'm going to just take the falciform ligament down just to minimize that risk with the LigaSure device. This can be done relatively simply with the LigaSure. You can probably do it - you can do it outside of it, it's okay. Yeah. For this case I like to use the the Maryland type LigaSure. I would think that the harmonic scalpel would be an equally good idea. The jaws are nice and small so when we do I lymph node dissection, this is a nice caliber in order to make that dissection more convenient Some of the larger devices, it can be challenging to to use those for the dissection I'll take this now to do this side. This will bring us down toward the first portion of the duodenum. I like to use a finer right angle instrument for the majority of my gastrectomy.
CHAPTER 4
So we're coming down now to the right gastroepiploic vein, which is this structure we see right here. And the right gastroepiploic vein, obviously, is going to go to the greater curvature of the stomach. We're going to ligate that. This is the middle colic vein and the middle colic vein joins the gastrocolic vein to form the gastrocolic trunk and the superior mesenteric vein is going to be deep to these branches here. So we're going to try to stay up high here - Well, not high here but we're going to stay obviously away from the colonic mesentery here and not injure these vessels. We're going to want to take the right gastroepiploic vein close to its junction with the gastrocolic trunk and harvest the station 6 lymph nodes, which live in this area here. Station 6 lymph nodes are perhaps the most important lymph nodes in a distal gastric cancer because they have the highest risk of metastatic involvement. Is that because they're usually right next to the tumor? Because they are next to the tumor, yes. Okay, 2-0 silk tie, please. I’m going to tie that one up, and I’ll clamp down. I'll grab the specimen for you. You certainly can use the LigaSure device for this. Sometimes for larger vessels I choose to clamp and tie them the old-fashioned way. It's good for the residents too, for training. Tie. Thank you. Gently now, these veins can be somewhat fragile. The next structure we're going to see is going to be the right gastroepiploic artery. This is just fatty and lymphatic tissue. I’m going to pinch burn that - might be a small vessel. That's a small vessel branch there that may be with the retraction - avulsed a little bit. This is carrying the dissection up to the first portion of the duodenum. D2 lymph nodes in this case would include stations 8, 9, and 11. The station 7 nodes importantly, which were formerly considered to be D2 nodes, are in fact D1 lymph nodes, and indeed the station 7 nodes at the left gastric artery, should be included in any gastrectomy as well Their metastatic rate is high on the order of at least 15 to 20%. That's higher than I'd expect. This patient has an early gastric cancer. He's elderly. One could argue not to do a D2 dissection at all in this case, so I'll probably just do sort of a D1 plus and take out the nodes at highest risk - maybe in stations 8, 9, and the proximal splenic nodes. Give me a Bovie here. Cause often, to take out all the splenic nodes, you have to do a splenectomy. Well I certainly wouldn’t go out to the distal splenic artery and the station 10 nodes. The likelihood of those being involved is incredibly low - and the morbidity of taking out those notes exceeds any benefit that you derive from taking them out.
So this is going to be the gastroepiploic artery. What’s our cautery on? Seems a little hot. 35. Can we turn it down to 30, Kathy? Sure. It's at 30. Great. Do you suture ligate this? No. Okay, 2-0 silk tie. We're gonna tie that one up - clamp below - with a little extra tissue here, but... Metz. Remember it’s a right angle so you have to - there you go. Okay. I'll take a tie on a pass. The right gastroepiploic artery comes off at the gastroduodenal artery right on the surface of the head of the pancreas. You want to take this artery close to its origin in order to fully resect the station 6 nodes.
You can hold that Andrea, and I'll take this. Just complete our dissection here in the infrapyloric area. Sometimes I try to get away with just buzzing things for speed, but then that leads to a little bleeding so…
Here's the cancer here I think - it’s very distal. Yeah there's a little thickening. Not super obvious. No. Sponge, please.
These are just some adhesions of the omentum to the gallbladder. Right angle. So now I'm clearing off the first portion of the duodenum. It’s just an omental adhesion to the anterior wall of D1 and distal to the pylorus. The tumor is located right here actually in the prepyloric antrum. It’s a subtle tumor, but it's easily palpable here. Measures maybe one and a half or two centimeters. So we're going to be able to do a fairly distal gastrectomy in this case.
CHAPTER 5
Right now I'm opening up the lesser omentum. And see how you can see that I'm circumferentially around the distal stomach and duodenum.
We’re going to do some of our superpyloric dissection here. We're going to take the right gastric vessels. Righties are station...? Right gastric vessels are the station 5 nodes. There are really very few lymph nodes in the station 5 location. In fact some autopsy studies have routinely found that there's no lymph nodes in station 5, but so I don't do a very aggressive proximal division of the right gastrics by the hepatics. I tend to take them fairly close to the stomach. I think we can probably just use the LigaSure device here. Okay. LigaSure? Thank you. And Heidi, do have the Endo GIA stapler? We're going to want a 60-mm tan load.
Maybe we'll clean this up just a touch here. Sorry Andrea.
CHAPTER 6
Okay, we’ll take that stapler. So we're dividing the duodenum now. I don't always do my gastrectomies in exactly the same steps. I kind of just go with whatever seems easiest at the time, so in this case, we entered the lesser sac, we mobilized the greater omentum. I didn't go leftward first. I went rightward. We took the right gastroepiploic vessels and the station 6 nodes. We then took down the lesser omentum, divided the right gastric vessels. We're now going to transect the duodenum distal to the pylorus. The pylorus is easily palpable as a ring. You want to make sure you take at least one to two centimeters of duodenum as a margin. His tumor is located here in the antrum, in the prepyloric space, so if we divide the duodenum there, that will give us at least a two- to three-centimeter margin. Articulate that. Your choice of stapler here is really personal preference. We've largely gone to the Covidien tri-staples. Do you want me to go in a little more there? Let's see, yeah, advance that slightly. Perfect. This fires three rows of staples on each side. Okay, ready? Go ahead. Yeah. No. 60 purple next.
So there's the duodenal stump now. I do not routinely oversew the duodenal stump - that is a personal preference. In some patients, perhaps if they've had pre-op chemo radiation I might consider its - DeBakey forceps - but sometimes oversewing this stump with Lambert sutures and whatnot can be more meddlesome than helpful. So this is a well-perfused stump with three rows of staples. The incidence of leaks should really be quite low, so I'm going to leave that be. So now the stomach is divided. We've got our tumor here in the antrum.
We're going to complete our dissection leftward and then we'll be ready to do the completion of the gastrectomy. There is commonly congenital adhesions behind the stomach to the anterior capsule of the pancreas. We're taking these down now. The pancreas is coming into view quite nicely here. So now we need to make a decision - how far left we want to go. Again, we're going to preserve all the short gastrics in this case. We could consider just taking the left gastroepiploics. Cautery to me and a DeBakey. Just a second now. Here. Okay so now we want to make sure we pick up the stomach again just to follow our path. Hold that there. Oh my, quite a few adhesions here. Make sure that - that's hemostatic before it goes away. Looks good, huh? Okay. This part of the operation can frankly be quite a bit of a nuisance taking the omentum off of the splenic flexure. You certainly want to be careful not to injure the spleen, because as you know, the short gastric vessels derive their blood supply from the spleen and the splenic artery, and so if you injure the spleen then you have to convert the patient to a total gastrectomy if you have taken all the other named vessels. So really examining this - the tumor being so distal in this case, we really can do a fairly modest distal gastrectomy with more than an adequate distal margin. So I think we've done enough leftward dissection, and honestly, we could perhaps come through here. Alright, if you want to hold that up, I'm going to take LigaSure device, please. And I just come through the omentum and the gastroepiploic vessels with the LigaSure device For more proximal cancer, I would take some of the lower short gastric vessels but in this case given that this is such a distal cancer, I don't think that's necessary. DeBakeys. So let's come through here.
CHAPTER 7
Alright, so at this point, we're ready to divide the stomach, but I like having the stomach as a handle to do the dissection at the left gastric. We can tuck the colon away. One thing that can help with the dissection of the left gastric and the nodes is to place a moist lap pad. And a malleable gently on the pancreas. Oh his left gastric is a ways up there, isn't it? So the left gastric vein is located here. You always find the left gastric vein in front of the artery. And here's the artery. You can actually see a pulsating. He's nice and thin - it's not often that you see it so easily. And this is going to be the common hepatic artery here. It’s actually a bit calcified in him. You can feel that right there. So the station 8 lymph nodes live on top of the common hepatic artery, and then the station 9 nodes are going to be down here in the celiac axis. The station 7 nodes are here along the left gastric, and the station 11 nodes are going to be here along the splenic artery, okay? So we're going to open up the peritoneum here. We’re going to take the left gastric vein first, then we're going to take the artery and reflect the station 7 nodes upward with the specimen. Right angle.
So this is the peritoneum, which overlies the common hepatic artery. Oftentimes there's a large node here. Does it have a special name or just...? No. It's there. It’s just there. So this is part of the D1 plus lymph node dissection that we’re doing here now - taking the lymph nodes off of the anterior surface of the common hepatic artery. DeBakey. Bovie. Let's come here. Starting to see the left gastric artery come into view there, right here. Probably should be doing this with the LigaSure. As you can see, there's lots of little vessels to the nodes, which are a nuisance. Again for speed, I sometimes just try to get away with using the cautery, but then you have to be careful cause then you get into some bleeding and... Okay, go ahead. Convert to the pediatric sucker there. The caudate wants to come into view there. Looks like a little vessel in there... maybe. Cautery here, too. You can grab the node, here. Cautery. DeBakey. Baby sucker. Bovie. Suction. And, can you send that as a separate specimen labeled station 8 lymph node?
Let’s see if we can take our left gastric vein right here with the LigaSure device. This will help us a lot - get this out of our way.
Okay, right angle. Thanks. So here we see the splenic artery coming into view. So common hepatic artery, splenic artery, left gastric is going to be here. So we're going to dissect out this nodal packet here on the surface of the pancreas. Let’s get this little guy here. Bovie. Thank you. Okay. Right angle.
Let's open up the peritoneum here on the superior border of the pancreas. These will be the station 11 nodes. LigaSure device, I think. These are going to go as station 11 lymph nodes for permanent. Bovie. Next we're going to want actually a 45 tan. Really need to get this caudate out of our way. So here's our left gastric artery there. Cautery and get these nodes up with our specimen.
So to take the station 7 nodes, you do want to take the left gastric artery at its origin, which is what we're doing here. And we’re going to use this just as a handle to put the stapler. I like to take it with a stapling device. We’ll have to see if we have enough room. Yeah. If we don't, we can clear up a little bit more. Right angle. There you go. Let me take this off. Open. Can you see my tips, just to make sure... Yep. Okay, and now you make sure you haven't compromised the common hepatic or the splenic artery, which you haven’t. Okay, go ahead and fire. So this is a division of the left gastric artery at its origin. Scissors. Great.
CHAPTER 8
Alright, so now I think we can choose our site for division of the stomach. Can you pull your nasogastric tube back now? It’s a very important thing to remember of course - you don’t want to chomp through the nasogastric tube. How far back do you want it? All the way? I would pull it back to just the GE Junction - maybe 40 centimeters or so. So, that's at 38 right there.
Great. So before we do the division of stomach, let's just clear off the lesser curvature and these nodes we’ve worked so hard to get in station... So we’re going to take the LigaSure. These are the Station 3, and I don't go up as high as station 1, which would be all the way up to the GE junction. These are basically the branches - the more distal branches of the left gastric, up on the lesser curve of the stomach. In order to preserve the length of our stomach remnant, the amount of - of reservoir left, we strip these nodes down distally. So we still get the nodes, but we don't have to resect the actual stomach. There's our left gastric stump. So we're obviously going to take that with us - come through these nodes here. This is a bit time-consuming, but I think with patience it's worth taking out these extra nodes in many cases. We can always come back and get additional nodes that are... Can you put this with... You can put that with station 7, I think he's... Yeah. So next is going to be the 60 purple.
So now we're ready to do the gastrectomy. Can almost see a line of demarcation where this is ischemic. Okay, I'll take the stapler. So we typically with two firings of this - you want to hold down perhaps here on the stomach? Take one more of these in back. I do this in the manner of Hofmeister, so we have a transverse bite here, and now we'll take an angled bite up the lesser curve. And then we’ll do our anastomosis to the greater curved proportion of the stomach. And I - we may not make it. We'll see. We might need a - the other 45. I would get one ready. There’s a little itty bitty left. Yes, a 45. Hold that guy like this. Okay, and this is going to be distal gastrectomy, and I would like them to check the duodenal margin. Duodenal margin. Do you want to mark it? Let’s mark it with a stitch, just so there’s no doubt Laurie. Yes, right there. Was that going to be for frozen? Yes. Do you have a little irrigation, Endi. Grab this section before you start.
I’ll take a DeBakey, Endi. Alright, so now we’ll get hemostasis before we do our anastomosis - make sure there's no more nodes we want to take. Suction in here. See if we can get our caudate out of the way. It’s been a nuisance the whole case. All of the separate lymph nodes go for permanent. Or do you want to send it with it? What's your call? So this is a good example of a completed D1 plus lymphadenectomy the common hepatic artery here is exposed nicely, the proximal splenic artery here. This is the Celiac axis. Here's the left gastric artery divided at its origin. There’s still a bit of lymph node tissue. This is not a perfect dissection in which we've taken every node but certainly a very reasonable lymphadenectomy for an 80-ish-year-old gentleman with a T2 cancer.
CHAPTER 9
Alright let's oversew the lesser curve staple line. Can I have that Babcock back? We’ll take a 3-0 PDS and some bowel forceps. 1 hour. Thank you, Keith. Thank you. Alright, so let’s start here and... No. Thank you. So now we're getting ready for our anastomosis. We first oversew the staple line along the lesser curvature. It's probably not essential, but it makes me feel a little better to imbricate that. I do it in a running Lembert fashion with PDS. You're going to cut the shorter end about 6 mm or so. I'll take forceps too. Stray staples. So Dr. Mullen, for the anastomosis, how do you decide between Billroth I and II? That’s a good question. So - the main limitation for most cancers I see is that many of the cancers are too proximal. So you end up having to do a fairly large gastrectomy such that the ability of the duodenum to reach the gastric stump without tension is limited. There are some purported benefits to having a Billroth I because you maintain the normal physiologic flow of food through the duodenum, but you know it has the troubling side effect of bile reflux - perhaps worse than you'd see with a Billroth II. So - they both have their advantages and disadvantages. I rarely do a Billroth I although it's much more common in Asia because they have a lot of early gastric cancers in the distal stomach in Asia, so they have greater experience with it. We in the United States almost exclusively do Billroth II’s or Roux reconstructions. The reason I would do a Billroth II is he has a reasonably good-sized gastric remnant. If he had a really small gastric remnant, I'd be reluctant to bring up a loop cause you'd have really bad bile reflux. So in that case I would do a Roux reconstruction. But - the advantage of a Billroth II over Roux is that you only have one anastomosis instead of two so it's less time consuming and you can always convert a Billroth II to a Roux. Once you do a Roux, it's hard to go back and do much else. Cut the needle off. This you'll cut some 6-7 mm.
Okay, let's go get our loop of the jejunum. I like to do mine retrocolic. It probably doesn't really matter at the end of the day. The key here is to not injure the middle colic vessels, which you can see coming up here nicely. So we're going to come to the left of the middle colic vessels. There is typically a bare area here, which is where we're going to bring our jejunal loop through, so you can take the cautery and vertically incise the mesocolon. Right through the bare area there. Come up a little more north here. Yeah, that should do. And then you're going to find your jejunum now at the Ligament of Treitz. Here? Yeah, so we’ll bring up the loop of jejunum. You don't want your - this is going to be the afferent limb - it's the limb that brings the bile and pancreatic juices to the stomach. You don’t want your afferent limb to be too long cause it can kink and give you the afferent limb syndrome. So typically what I do and you can bring it up in isoperistaltic fashion or antiperistaltic fashion. Peristalsis goes in this direction, right? From the Ligament of Treitz distally. So the stomach contracts in this direction, so to bring it up isoperistaltic, you want to orient it this way. If you bring it up this way, it’s antiperistaltic, and truthfully, it's been studied - how you orient it really doesn't matter very much. And so I tend to just do it the way that it tends to lay nicely. And I make sure that the the limb is not too - redundant, so there's some snugness to it. Now we can take the colon away. Okay, Babcock. Now we have to go find our stomach remnant. So we decided - I want to make sure we check how we've got this oriented. This is afferent limb. This is the efferent limb. I think this will lay nicely almost here in antiperistaltic fashion.
Okay, before we do, let's place our corner stitches. So why don't you place your corner stitch there - antimesenteric portion of the jejunum. Now get a good bite. And now the stomach. Far behind - further behind the staple line - maybe not quite that far, but yeah - good. Cause when you excise the staple line, you don’t want to cut your stitch. Okay, snap. Alright and now let's do our other corner. So we’ll do it to there. Just come right under the staple line - great, snap. Need another. Snap, please. Right now we can get Mr. Colon out of the way. Put this in a little tension - see like that. Do you have a Ray-Tec?
Okay, now you put your back row of Lemberts in. I'll take bowel forceps. Great. Grab that guy. Stitch. Needle back. Stitch. These are Lembert sutures. They’re seromuscular stitches. Not a strength layer. Not a strength layer but - certainly could do this anastomosis in many ways - single layer, stapled - this is a more traditional two-layer hand-sewn end-to-side gastrojejunostomy. Outer row of silk, inner row of some sort of absorbable suture - some use chromic, some use Vicryl, I use PDS. I like the PDS because it's monofilament. Laurie, do you know what is the strength layer in a bowel anastomosis? I mean I think it has to go across the entire bowel wall There’s a specific layer. What’s the strongest layer of the four layers? Well there's mucosa, submucosa muscularis, I think it's the submucosa. That’s right. Excellent. We should probably do it I think. What do you think? You want to put another one? Probably. Alright. One more. Residents always want to put in lots. Alright, why don’t you start tying the corner there. We'll re-snap that one. Do you have the Yankauer sucker now? Why don’t you take the cautery there, and I'll take a Schnidt.
So now we're making our enterotomies - Make a jejunotomy here and then we’ll excise the staple line on the stomach. Alright, that looks good. Here we stay close to the staple line just to make sure we don't get too close to our Lembert stitches - accidentally cut them. Almost there, huh? Maybe heavy scissors there, and amputate that guy. Alright, some like to use it as a handle. I'm with you, I just prefer to use my forceps. Alright 3-0 PDS.
That’s perfectly fine. Yep, approximately the middle. Make sure you get all layers. Great and tie that one. 6 knots. And we’re going to cut this one about 6 mm. Do you have a shod, Endi? We just need one, actually. Great, that’s nice. Make sure you get all the layers. It’s easy, when it retracts, to miss it, and then you end up not getting the serosa of the stomach. Lovely. Shods are little plastic booties on the clamp that doesn't fracture the suture. The problem is if you put a clamp directly on monofilament suture, you’ll weaken it, and it could crack. And when you're using it, it can break. So we try to put shods. You’ll see them commonly in vascular surgery. They use a lot of Prolene, and they'll put shods on all of the ends of their stitch - their stitches. You don't see those much in GI surgery. Okay we're going to run this way toward you full thickness. Nice. Push the mucosa down with your stitch. Yep. So the only reason I check the duodenal margin is because clearly the tumor was much closer to the duodenum than the stomach. We had a very wide stomach margin - grossly - but the duodenum margin was perhaps only two centimeters, so I had them freeze that. For cancers that are right in the middle, you know, it’s reasonable of course, or for certainly diffuse type cancers - this is an intestinal type cancer - I'd be inclined to test on frozen section both margins. You must be using the epidural key. We have an active - we have a busy jejunum. That’s okay. We'll get through it.
Have you seen a hand-sewn bowel anastomosis, Laurie? I have not, it's lovely. Okay, there you go. So the corners can be tricky. There’s a technique called Connelling. To help it. It everts the mucosa. And now you’re going to go inside out on this side. So essentially instead of going across like you were doing before, so I went outside in so now I go inside out. And now I’m outside, so I'm gonna go outside in. I’m going to shod you at this point and then bring mine around. Hold that stitch. Bowel forceps. All layers of the bowel wall - it’s important to see that. Come around the corner, 45-degree angle, flip your stitch, and a 45-degree angle back. Lots of serosa - not too much mucosa. I will try and come out with a 90-degree here. Flip your stitch. I think I got more mucosa than I needed there. It’s okay. And a 45. It's getting easier now. It's pooching back in - there you go. In a second, we're going to have you advance the nasogastric tube. One more - well, two more I guess. huh? Have to get to the other side. Grab the serosa, so you can pull the small bowel out. That’s mucosa there, yep. Yep. Okay, we'll take the scissors. Cut the needles off. Yep, great. Okay now we’ll take silks. And now we do what we did before.
As we get over towards the lesser curvature portion of the anastomosis, this is actually historically called the angle of death - or the angle of sorrow - because this used to be a frequent site of leak - because it is a site where there's a little more tension, so we're going to put a few extra stitches in here. That should do it I think. That is a lot of silk. Alright. Okay. Alright. Okay. Should I cut this too? Oh yes, yep, you have this one here. Shorter if you can.
The nasogastric tube. Go slow. Okay. Yeah, I don’t feel you. Oh, there you are. Great. Keep going? A little bit more. That’s great. So I’d leave the nasogastric tube in the gastric pouch cause that's what you really want to decompress. It's not so important to put it down into the efferent limb, because you're not going to get anything out of there anyway I just try to keep the gastric remnant from blowing up and the risk of aspiration. And I usually leave that in for one or two days depending on how concerned I am with the anastomosis. I don't usually do a swallow. Probably just take it out on the weekend and start him on liquid.
CHAPTER 10
Hemostatic, a little juicy here - how about some warm irrigation? Maybe a... A DeBakey. Here you go. Grazie. I'll grab a DeBakey as well, please. Thank you. Aha, it's here! Those lymph nodes. I’ll take a longer DeBakey. Station 3 lymph nodes for permanent. These are some additional nodes - they’re sort of high up on the lesser curve - whether you call them 7 or 3, I don't know. Perhaps they’re better termed 7, but… Sometimes these are just easier to take out once the specimen is out. I think I would just amputate right there if you can I know it's not an angle on this but - Yes. Tiny bit more. Yes. No - that - that is the location. Yeah. Okay so here's the ligated left gastric artery at its origin, okay? This is the aorta here. This is the - so this is what we call the celiac axis cause it's the trifurcation - splenic artery here, common hepatic artery here, so the left gastric comes up. Additional station - you can call it station 8 lymph node. Yeah. Sorry, I - hate giving you to - these to you in bits, but... Bovie. So I just put it together with the first number, station 8 - Yes, that'd be great if it hasn't gone already, yeah. Thank you, beautiful.
Yeah we have to close this because if we don't, we get a hernia - we could get a hernia. Where the bowel will herniate up into the upper abdomen above the mesocolon. So we close this. This is a big problem in patients who have gastric bypasses who have done retrocolic, and if this defect isn't closed, they can have strangulated bowel that herniates through here. Okay, pop that off and tie it. You want to secure the cut edge of the mesocolon to the stomach, and that's just because you don't want to narrow your anastomosis or the efferent limb. So you pull the anastomosis below the mesocolon and then just with a few interrupted sutures. Needle. Thank you. Another stitch.
Actually, we have that - xiphoid is here, so there's the fascia of Wight. I want you to get up - just a second, sorry. Relax here - way up here. Good. What are the chances we’ll have to do a thoracotomy? Well I just think it’s so hard to get there in supine. You’re coming - you want to come out more. Yeah. Because your last stitch came out here. Yes. Better. If it were someone like thinner, do you think you could do it supine? Oh I could, for sure. Yeah. Well there were two reasons I wasn’t thrilled about doing it that way. One was that she has a big hernia, so then we’d have to fix her hernia - probably with mesh so that just adds complexity to the case And that doesn't bother her - she doesn't care if it's fixed, so I said fine. And then the second thing is - I told you, she's - the location of this tumor is terrible. Make sure there’s no purple there. Okay, good.
No, it's fine. Which way - can you staple from this way?
CHAPTER 11
I think in general the operation went well. As is common with the lymph node dissection, there a lot of little vessels to the nodes and that's where we got into some little bleeding - not significant, but enough to be a nuisance. So that adds time. I probably should have that little LigaSure device more frequently, but that takes more time cause you have to exchange instruments frequently. So I try to just go as much as I can with the cautery, but then sometimes you buzz through a vessel, it bleeds, and then it takes more time. So - that sort of is just the nuisance factor of taking out nodes in this area, and that’s why a lot of surgeons don't want to do it frankly, because it adds extra time and - and complexity. But it’s not necessarily hard - it just takes a little patience to do it. So I probably could have got a little better job with hemostasis there if I used the - the vessel sealing device more frequently.