
Arthroscopic Acetabular Labral Repair
Main Text
Table of Contents
- Describe the onset of symptoms. Was it insidious or was there a preceding event?
- What is the location of pain?
- What is the quality of the pain? Are there any mechanical symptoms, such as a pop, snatch, catch, lock, or subluxation/instability?
- Is there exacerbation with sitting?
- Is pain activity-related?
- What relieves the pain?
- Do you walk with a limp?
- Do you have limitations to walking a distance or climbing stairs?
- Hip range of motion may be similar in the affected and unaffected hip.
- Assess flexion and internal rotation, comparing the affected and unaffected hip. The unaffected hip may exhibit reduced flexion and internal rotation or pain with range of motion.
- Assess for Trendelenburg sign by having patient stand on one leg on the affected side. The test is positive if the pelvis drops on the contralateral side. This occurs in 33% of patients with femoroacetabular impingement.
- Perform anterior impingement test by passively flexing the adducted hip and slowly internally rotating. This test reproduces anterior groin pain in 88% of patients with femoroacetabular impingement.
- Perform FABER (flexion-abduction-external rotation) test.
- Perform resisted straight leg raise.
- Perform log roll test. Pain is reproduced in 30% of patient with FAI with log roll test.
- Perform posterior impingement test by placing the hip in extension and external rotation. Hip pain is reproduced in 21% of patients with FAI with posterior impingement test.
- Perform a complete exam of the affected limb and lumbar spine to rule out bursitis, nerve entrapment, and referred pain.1,2
- Lateral Center Edge Angle: the angle formed by a vertical line drawn from the center of the femoral head and a line drawn from the lateral rim to the center of the head. An angle less than 20 degrees indicates dysplasia.
- Acetabular Index: the angle formed by the acetabular roof or sourcil. An angle greater than 10 degrees indicates dysplasia.
- Acetabular Version: Traces lines from anterolateral acetabular edge along anterior and posterior projections of acetabular rim. An anterior wall that is more lateral than the posterior wall (“Posterior Wall Sign”) indicates retroversion. An anterior wall that crosses the posterior wall (“Cross-over sign”) indicates bony excess at anterior rim and relative retroversion.
- A cross-table lateral view is important for assessment of femoroacetabular impingement, allowing a view of the anterolateral femoral neck.
- Alpha-angle: Formed between a line along the midline of the femoral neck and a line from the center of the femoral head to the point where excess bone deviates from normal femoral head sphericity. An angle >60 degrees indicates femoroacetabular impingement.
- Head-Neck Offset: Begin with a line bisecting longitudinal axis of femoral neck. Draw a parallel line that is tangential to the anterior aspect of the femoral neck and measure the distance to a parallel line tangential to the anterior femoral head. Normal distance is >9 mm or a ratio to head diameter >0.17.
 Pre-oerative AP Pelvis
Pre-oerative AP Pelvis  Pre-operative AP Right Hip
Pre-operative AP Right Hip  Pre-operative Lateral Right Hip
Pre-operative Lateral Right Hip  Pre-operative Sagittal MRI - T1
Pre-operative Sagittal MRI - T1  Pre-operative Sagittal MRI - T2
Pre-operative Sagittal MRI - T2 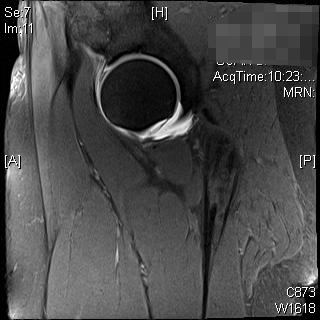 Pre-operative Sagittal MRI - T2
Pre-operative Sagittal MRI - T2 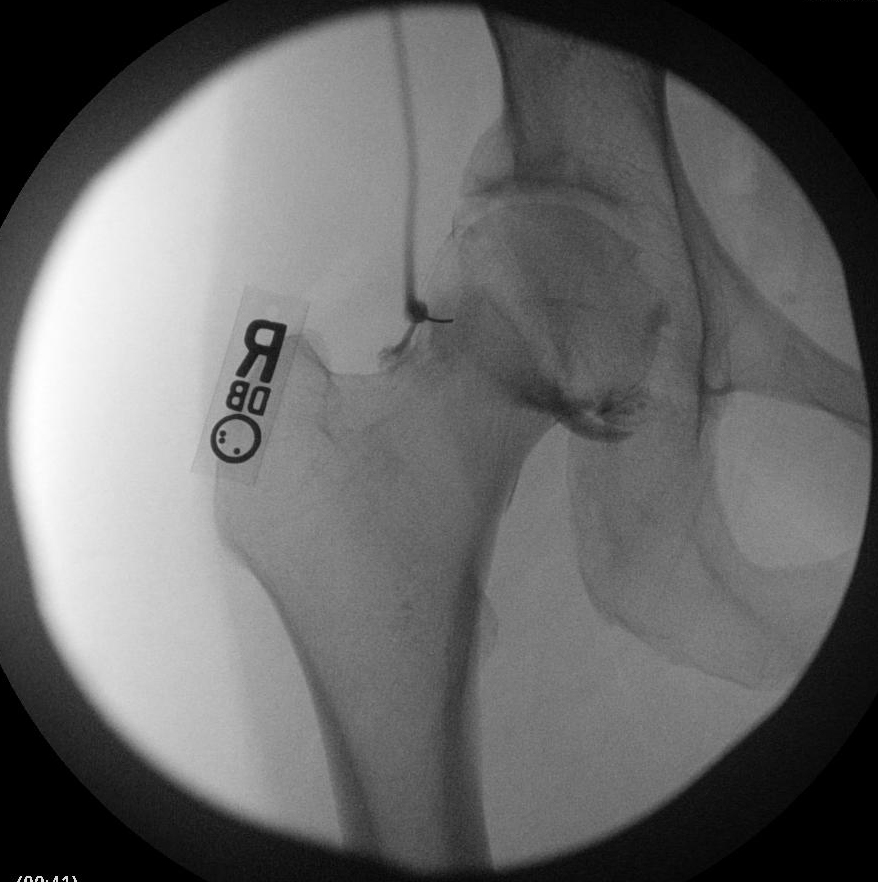 Intra-operative C-Arm AP Right Hip with contrast
Intra-operative C-Arm AP Right Hip with contrast Intra-operative C-Arm AP Right Hip with contrast
Intra-operative C-Arm AP Right Hip with contrast  Intra-operative C-Arm AP Right Hip
Intra-operative C-Arm AP Right Hip  Intra-operative Lateral Right hip
Intra-operative Lateral Right hip 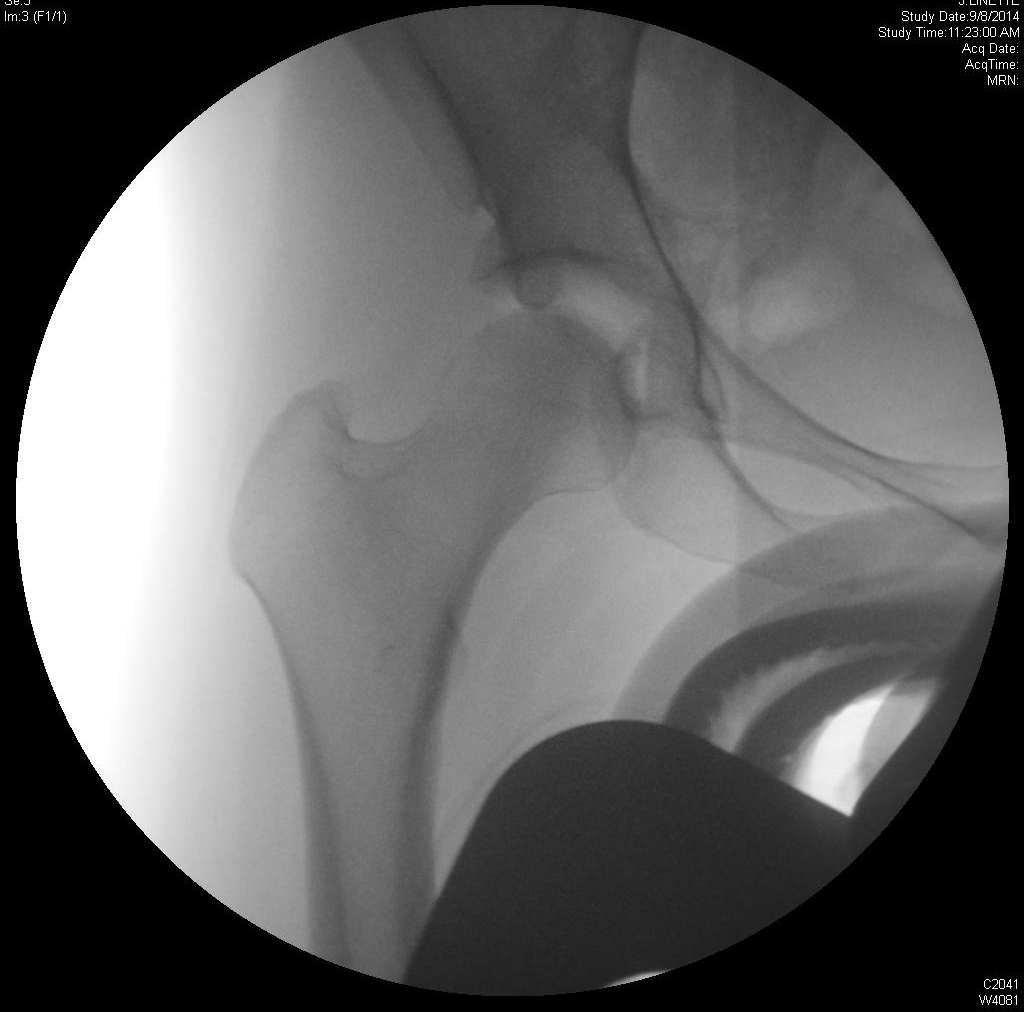 Intra-operative AP Right hip
Intra-operative AP Right hip 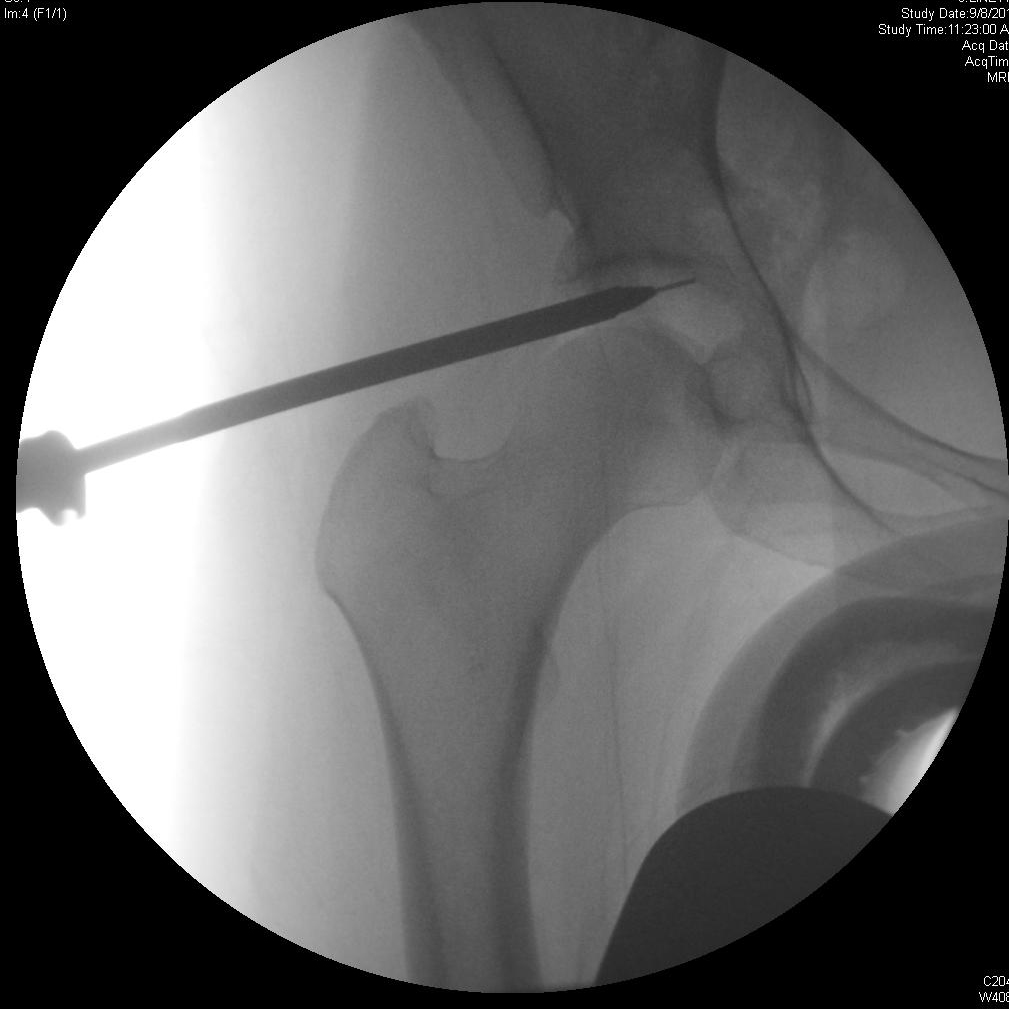 Intra-operative AP Right hip
Intra-operative AP Right hip 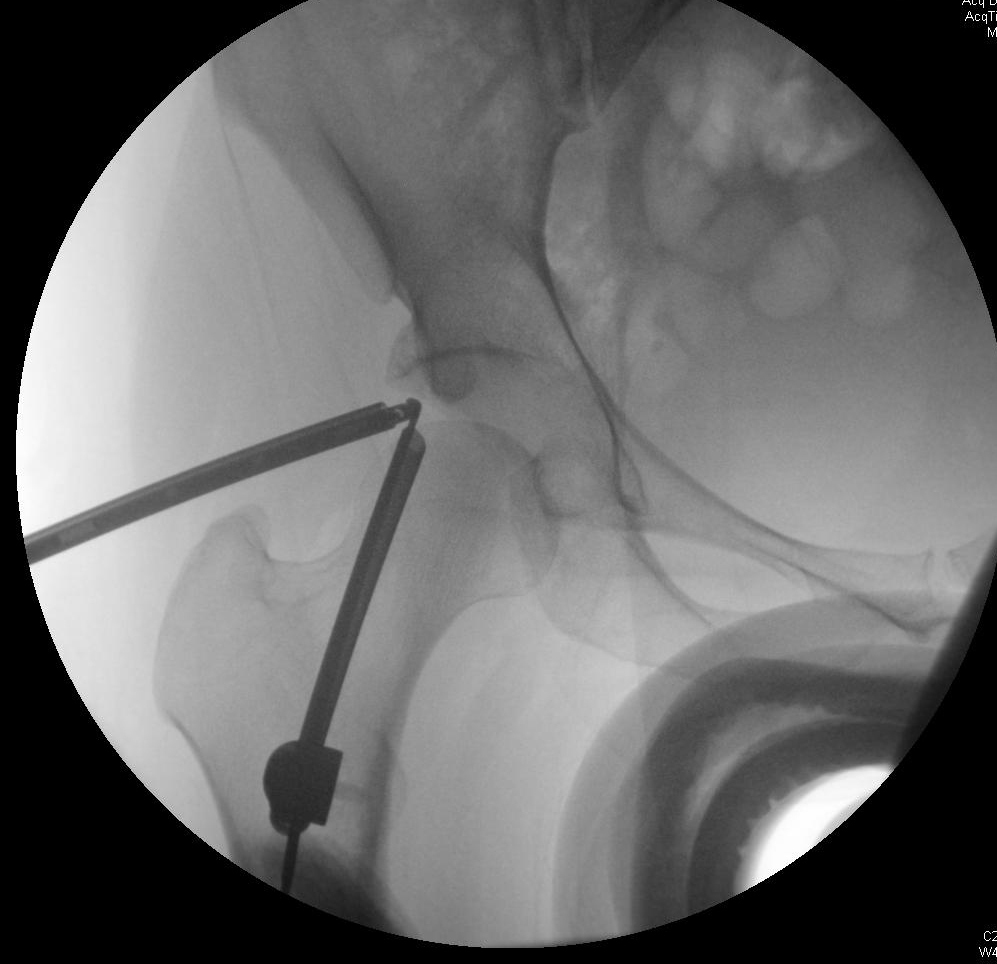 Intra-operative AP Right hip
Intra-operative AP Right hip 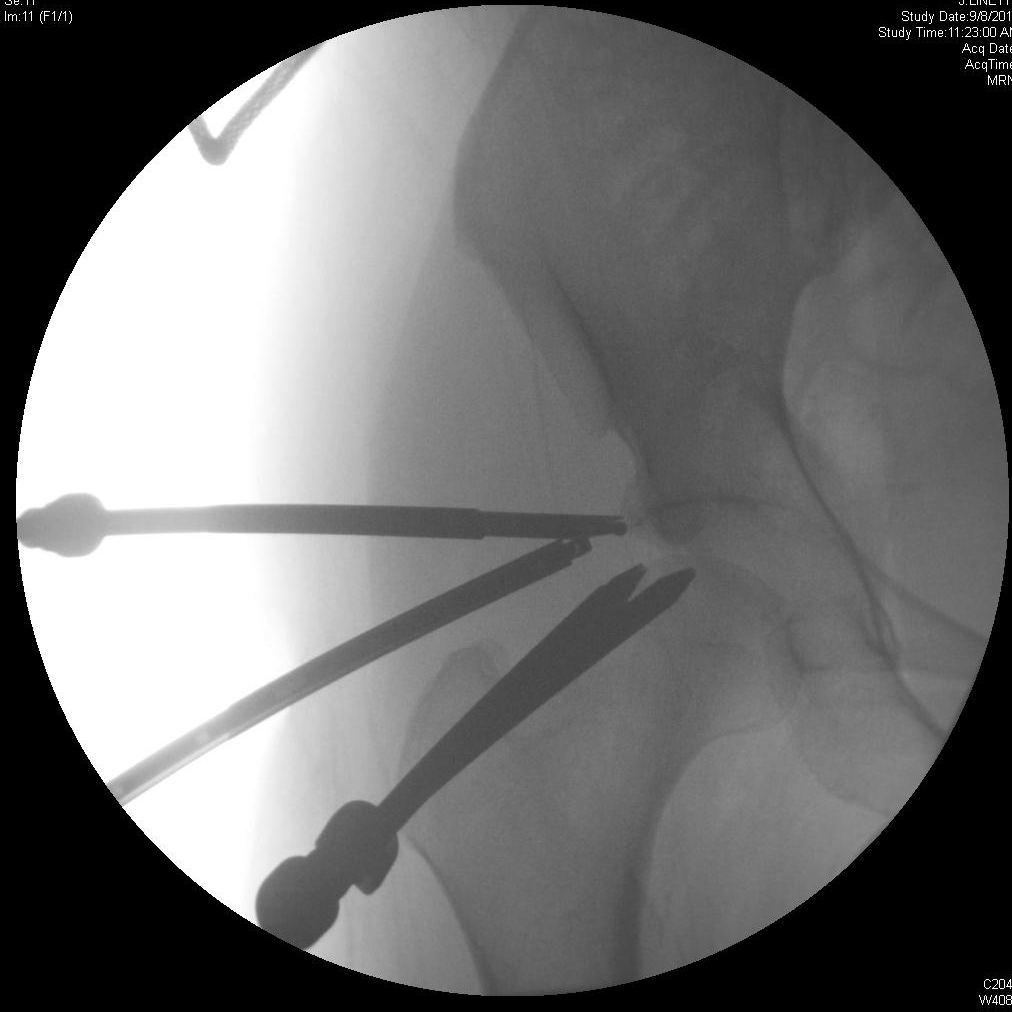 Intra-operative AP Right hip
Intra-operative AP Right hip 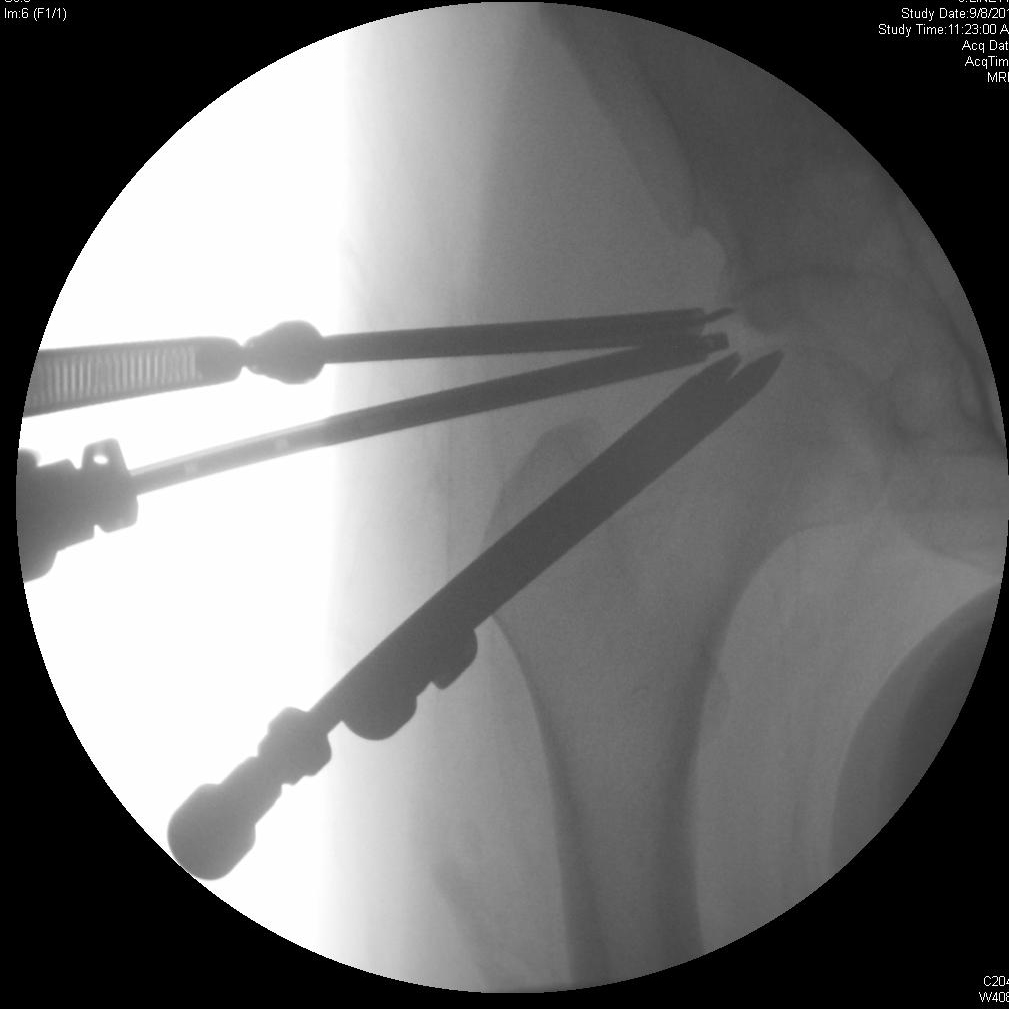 Intra-operative AP Right hip
Intra-operative AP Right hip  Intra-operative AP Right hip
Intra-operative AP Right hip - Knife Rasp, Smith and Nephew
- 2.3 Bioraptor Osteoarticular suture anchors, Smith and Nephew
- #2 FiberWire sutures, Arthrex
Citations
- Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res. 2009;467(3):638-644. doi:10.1007/s11999-008-0680-y.
- Guanche CA, Bare AA. Arthroscopic treatment of femoroacetabular impingement. Arthroscopy. 2006;22(1):95-106. doi:10.1016/j.arthro.2005.10.018.
- Ilizaliturri VM Jr, Orozco-Rodriguez L, Acosta-Rodríguez E, Camacho-Galindo J. Arthroscopic treatment of cam-type femoroacetabular impingement: preliminary report at 2 years minimum follow-up. J Arthroplasty. 2008;23(2):226-234. doi:10.1016/j.arth.2007.03.016.
- Philippon MJ, Stubbs AJ, Schenker ML, Maxwell RB, Ganz R, Leunig M. Arthroscopic management of femoroacetabular impingement: osteoplasty technique and literature review. Am J Sports Med. 2007;35(9):1571-1580. doi:10.1177/0363546507300258.
- Maheshwari AV, Malik A, Dorr LD. Impingement of the native hip joint. J Bone Joint Surg Am. 2007;89(11):2508-2518. doi:10.2106/JBJS.F.01296.
- Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res. 2004;429:170-177. doi:10.1097/01.blo.0000150119.49983.ef.
- Larson CM, Giveans MR. Arthroscopic management of femoroacetabular impingement: early outcomes measures. Arthroscopy. 2008;24(5):540-546. doi:10.1016/j.arthro.2007.11.007.
- Philippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: minimum two-year follow-up. J Bone Joint Surg Br. 2009;91(1):16-23. doi:10.1302/0301-620X.91B1.21329.
- Larson CM, Giveans MR. Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement. Arthroscopy. 2009;25(4):369-376. doi:10.1016/j.arthro.2008.12.014.
- Kelly BT, Weiland DE, Schenker ML, Philippon MJ. Arthroscopic labral repair in the hip: surgical technique and review of the literature. Arthroscopy. 2005;21(12):1496-1504. doi:10.1016/j.arthro.2005.08.013.
- Stalzer S, Wahoff M, Scanlan M. Rehabilitation following hip arthroscopy. Clin Sports Med. 2006;25(2):337-357. doi:10.1016/j.csm.2005.12.008.
Procedure Outline
Table of Contents
- The patient is taken to the operating room and positioned supine on the operating table.
- The patient is placed under general anesthesia with endotracheal tube intubation.
- The patient is then placed against a silicone-padded perineal post, in foam boots and placed in traction.
- A positive vacuum sign is noted after which traction is let off.
- The patient is then draped and prepped in usual sterile manner using aseptic technique.
- The anterolateral portal is established using fluoroscopic guidance with the gauge cannulated needle and the joint insufflated.
- A 5-0 obturator and cannula are then placed.
- The anterior portal is established next under direct arthroscopic viewing.
- This is followed by the mid anterior portal and Dienst portal.
- A diagnostic arthroscopy is performed to assess the surrounding structures, including the labrum, Ligamentum Teres, Pulvinar and Femoral head.
- The acetabular rim is then recessed using fluoroscopic guidance, starting laterally and working medially from approximately the 12 o'clock to the 3 o'clock position using a #4-0 round abrader on reverse.
- Labral repair is undertaken by visualizing the transverse ligament, then cleaning the inferior recess and acetabular notch of any loose bodies.
- Accessory mid-anterior and Dienst portals are then used to introduce the Smith and Nephew knife rasp to elevate the capsule approximately 5-8 mm above the capsulolabral junction, then cut down to the acetabular brim.
- Anchors are then placed with 2.3 osteoarticular Smith and Nephew anchors.
- The sutures are shuttled through the labrum using vertical mattress sutures and each anchor and suture is passed the same under direct fluoroscopic guidance along with direct viewing.
- Knots are tied on the capsular recess side using a modified Weston with multiple half hitches, using vertical mattresses.
- Sutures are shuttled using wire suture shuttle relay and the anchors are composite 2.3 osteoarticular anchors loaded with #2 FiberWire sutures, again knots were kept on the capsular recess side.
- In addition, the labrum is tensioned down with the traction let off so as not to evert the labrum and also to reconstitute the labrum back to its newly recessed acetabular rim.
- Tissue is then tested for stability of repair by probing.
- The hip joint is put through range of motion to assess stability.
- Traction is then let off.
- The instruments are removed and the scope is placed in the peripheral compartment.
- Medial and lateral gutters are assessed for presence of loose bodies.
- The medial and lateral synovial folds are assessed for lesion.
- The Zona orbicularis is assessed for lesions.
- The capsular reflection is assessed for separation off of the femoral neck.
- The scope and instruments are removed.
- The portals are closed using 3-0 nylon sutures with interrupted stitches and then covered with Adaptic along with sterile gauze along with Op-Site dressings.
- The patient is awakened, extubated, and transferred to recovery room bed and checked post-operatively for any surgical complications.
Transcription
CHAPTER 1
So there's the top of the troc right there. So what I'll do is I'll put my finger down here, and I know that that's the posterolateral portal, and then she's tiny, so I’d bring her down to here. Yeah, then straight across, this way - you always want to see that pubic hair line cuz that'll give you exactly where the joint is - I’d say we’ll be somewhere in here - about here.
Now she has a pretty big tear, so our big problem is when he goes in, the area of the tear extends right into our portal, so if we get on the inside of that labrum, it's going to be like a bucket handle tear it’s going to follow us around, and we’ll be blind. So we we got to try some how to get on the outside at labrum, so it's maybe 2-3 mm difference, you know, whether or not you’re dragging the labram around with you, or whether he gets a clean stick here.
Good inclination - looks pretty good. So one turn on that side - we’re going to do traction - 5, cuz that took everything off. Yep, a lot of this is viscoelasticity in the system, so it's not really traction on the joint. It's her tensioning up against our silicone pad on her post. It's her tensioning in the boot before we ever see traction here. Does 10, 5 more. Okay, good. Yep. And he wants to be in about 15 to 20 degree inclination for us to be able to work, because remember, we're coming into very constrained joint, so at increased working distance we want to be right in line with the joint. If we're too perpendicular to the joint, then it’s very difficult for us to work with that portal as an utility portal. We can view, but it's very difficult to use it as an utility portal.
Just to get the - change the inclination on your needle. Yeah, yeah, I always think about picking your hand up like this, and when you change directions, you got to come all the way back out. Keep her hand up even more. Keep posteriorly. And as you’re ready to perforate the capsule, you got to just watch the inclination and that your - you've got at least 15 degrees.
Yeah, I think you need to be right off of that head. We’re going to be fighting with this. John have some fluid ready - well did you perf? It looks like you're almost in - looks like you're in Alice. Does it feel like you're in? You like the last one? No - so just try some fluid if you think you're in. Let's see what your outflow is. Yep now, do your nitinol wire. It’s okay - she was soft stick. Go with your nitinol wire. If it’s in, the nitinol wire should hit your medial wall. So he's bumping against the medial wall of the acetabulum. Good, yep, make your incision. Make one spot there. Good. He could still be through her tear cuz it's a big tear, so it doesn't stay on the edge of the acetabular rim it goes like this, and so it's very easy for us to get inside of it. And we have some tricks to get around that eventually. 99 wire.
There’s two places that he's going to tether right here at the skin is going to be probably the toughest one on her cuz her capsule is thin. In older patients, I'm telling you, the capsule gets very thin, and younger patients, like if they’re 15, it’s unbelievable how thick it is. You got to keep your hand up. Remember, you went in with about 10 degrees - you want to be collinear - just make sure your collinear - make sure your obturator is locked out in the cannula. So he has to make sure that that wire doesn't start to bend or he can be having a straight wire like this and he's cutting across it this way.
It tethers - make sure that you hold and pull out the obturator with the wire, so if it tethers, we know that the wire is wrapped around the head. If he tries to pull the wire back, he'll break it right there. If he loosens up the obturator and brings the wire and the obturator back, it'll come right back in. The big thing is if it tethers, you do not want to force it through, because it's a teeny little opening - it’s only enough for that wire. If it's bent, it won't go through - it'll break.
You should be in. Yep, so we’re going to… It’s just a, yeah, it's a big floppy labrum. Lot different from the last patient. Yeah, big difference. You want that cross-sectional line in line with this. So I’m - I’m just going to show you here. So I would say the cross-sectional line is more like that, so I think you're right on that point, yep.
He’s looking at this triangle right here, see the capsule forms a triangle. And not unlike the shoulder where you have a safe triangle to get in, right above your subscap, and get the femoral head on your right, labrum on your left, this red stuff up here is the capsule that we're trying to get through - we are trying to get through right in the center of that cuz I'm going to have to put other obturators in - he needs to be right in the center of that.
Laterally, and I always back up so that you're not bending that needle. This one has to be right on because I have to use it as an utility portal. So come up lateral just a little bit more. So see how tight the head is over there? If he goes in with a cannula there, he's going to scab the head. When you come in here, where it's opening up, there's more space. If I come in over here, and it's closed down, so if I try to force the cannula between the acetabulum and the femoral head, he's going to skive there whereas here it's opening up like that. You can see this whole area opening up with the apex of the triangle being medial.
I want just a little more superior - yep. A little more distal and then you can go a little more lateral - yep, you got. Go ahead and make a small slit. Need to take a picture of that. That just shows you - yep - and so every time that wire moves and it's not - and it goes off to the side on at angle, you know that you're pushing in the wrong direction. Stay here with that - yep - cuz these wires will break. Remember, you're not - you’re not coming in with your obturator or with your cannula - just coming with just - just to there, yeah. Then take your knife, and just do a little slit on the capsule.
So we make a little slit in the capsule just to relax it, so we're not putting too much pressure on the head. And the head will see some indentation - it's like a ping pong ball - only thing is it because it's elastic defamation, it'll come back - plastic defamation, it’ll come back. So if you came back the end of the case, the - that defect would be gone. She doesn't have one yet, but she will. Just a little like a millimeter here and then a millimeter medial. So see unlike the other one, see how your knife is able to stay vertical without you angling it? So this way, if I got to retrieve my suture or anything else, I can use this as an utility portal. Perfect stick.
From out here, and you're trying to hit a 5 mm patch inside, a very small region for error, so he's right on it. Now we're going to open this up - come on over here, Drew, to make a viewing portal. So we're going to make this not only viewing but also for utility - for passing anchors, sutures, what not - I’m going to take the mytech - and this is what trying to keep it down even below the capsule so the cartiledge doesn’t take a hit. We use high flow rate. People take a knife, and they just cut this all the way. I don't think that's a good idea. Couple reasons: one is heterotopic ossification, which we see quite a bit on referrals - right here, take a look over.
So this is a transverse ligament right here where see the labrum is right here, and then that little defect going up here, that's the acetabular notch right there. You can see a little bit of discoloration - that yellow discoloration we talked about - and that looks good. Our pulvinar, our ligamentum teres again, right here on the right. Pulvinar there. And this anterior portal is good for viewing just the opposite direction, so anterolateral, inferiorly. Now we’re going to switch back cuz most of what we want to do is up near - from this portal here all the way up to our anterior portal, so we’re going to flip back to the other side.
This whole thing is disrupted here - all the way came in - all the apartments. May I have the obturator? So now I’m going to make some accessory portals - they’re going to be a mid-anterior portal. You look at this, it’s almost going to be an isosceles triangle. I’ll take the needle. We came in here so that we can drill through it, and we can pass our sutures and things through it without getting constricted. Most important, our anchors have to go to this portal. So we're angling toward the acetabular rim to get this one in, so we could put our anchors right in the rim.
Call it a dienst portal - I come from the ASIS right here, and I come down about one-third to one-half of the way, and it's going to make me a quadrilateral space right here to work through. This is going to be for passing sutures and doing our acetabular recession.
This is what I told you about right here - right - right at the capsule labrum junction where the labrum meets the capsule. Right here, that's where main blood supply comes in, so we don't want to take a knife and come through there. We want to come up above it, so I've got some capsule in here - all this stuff here - and we're going to use that to augment her labrum for her labral repairs, so my sutures don't pull through.
CHAPTER 2
I swear, we got to be really careful elevating this up. Okay Drew, tap, tap. Tap that. And we try to elevate up with just from this portal here all the way up to our anterior portal, so we're going to flip back to...
So this the rim that we’re talking about right here, labrum. This fibers right here are the deep head of the rectus. Let’s have a 4-0, round debraider, 4-0. Okay. You’re going to feel it right here, right here. Okay, you’re just going to flatten that out. She’s got soft bone. This whole area and then that deep head of the rectus isright here. So come from here, just nice and easy come down, counterclockwise. So we use intermittent traction now because we're up in the peripheral compartment, so counterclockwise, we're going to need that. You can take off five, and then take a spot when you start - spot here - get back off now. We don't need it to go any further than that there, and I'm going to bring you up here. So here's your labrum. Here's your chondrolabral junction. You’re coming all the way up here.
Soft bone - soft bone - you’re digging in big guy - you don't want to do that. Just want to scarify it, okay? She's got soft bone. You’re never going to get those anchors to hold. So that's already done. So right - and then you can take a spot - and keep working, keep working though. We’ll take a spot with you’re working. Yep, come in a lil bit more, good. Right there. Spot there. Keep working.
Now if she were younger, see how easy this is coming off? That's on reverse. I would be very aggressive at taking that all the way off. With her age, I think it's a mistake - to God she doesn't see this video. Turn a little bit more - another spot there. Drill - tap first - drill. In the anchor - get her. Not easy - go all the way down - all the way - all the way - out though. Suture grasper.
So this is my own technique. The needle is small needle, and the problem with the suture shuttles and the passthroughs for this is that they create a lot of damage they are big number 1. Take the needle out. Okay, hold that cannula. This one - I’m in. Okay, Sam went through. Sic. Okay, now needle. Now remember you’re going to hold both sides. You’re going to hold this up and that up. This is a saddle technique. And this one tight - that’s the way. I’m going to go oblique. Felt good. Okay. Good. Yep, yep.
Now your loop is going to go through. This a vertical mattress. Pull back. Yep. Needle out. Okay. Send that through. This is our own technique - minimal perforation. If I use some of the sharp penetrators, it would have a big hole in this labrum - there's no way you could put a vertical mattress in. So we just will take 5 off.
So now we're going to pull our back limb that went through our bone, so if I pull this limb I can giggly it through this whole labrum and cut it in half right here. They don't call it a fiber wire for nothing. It's made out of the same substance as Kevlar vests, but it can cut our fingers so it can cut right through that labrum. So we need to get it moving first cuz it's - remember, that anchor is deep inside bone, so I do the back limb here. Pull it up on this side first to get it moving to make a track, and then I pull this through - it comes back much easier. And we want our knot on our back limb so it's recessed back here off of the joint surface.
I don’t know if you've seen those, but they're big and they really decimate the whole labrum if you pass just one pass through. It’s disgusting. I think we're going to go to smaller anchors, which they're trying to do now - your 1-7 I'm mean we’ll be out when you guys keep promising me. And cuz the problem is not going to be in the suture of the anchor usually once you get it in. Pulling it out when you’re putting it in can be a problem. Once you get it in, the rate limiting factor is the healing of a labrum back.
Now I’m going to let all of our traction down. We let the femoral head reduce the labrum back to the rim. So I got to get that to flip now. There it goes. Scissors. For this to look like that, the question is can I do an all vertical mattress - I don't know. I don't know. Drill up. We’re going to - you have your second one opened up, right? There’s one. We’ll come right here for our other one - right on the edge of the rim right here. Go ahead, tap, tap. All the way down. Suture grasper. Pull up both sides.
So he's got the back in here. There's my one limb. There's my other rim. And he's giving me some tension, so I can grab as much tissue in here as I can as it allows me to. I'm going to go slightly obliquely - try to pick up more tissue. Five.
So what we want to do is, we want the hip, the femoral head, to reconstitute the labrum back to the acetabular rim, and we just did an acetabular recession. So now, instead of being here, it's back here. If I just drill holes and put it on, it can be evert, even if it's off a millimeter or two. We use the femoral head to reduce the rim - reduce the labrum back to the rim - and then we tension it so that we don't evert it. We do it with the traction all the way down, labrum is all the way back. We're not going to evert the labrum up like this if we over tension it. Why? Because of traction reduced the femoral head back into the socket. We did two different things. One is we're putting the labrum right back to its new recessed rim, and two is we're not allowing it to evert with over tensioning when we're tying it down cuz it's very easy for me to over tension and pull the labrum right up like that.
So this is a sliding knot, a modified Weston. It really takes it down, and we borrowed some of that capsule to augment our labrum so that this doesn't pull through. And now Drew is going to show me a reduction to take all the traction off now. So I'm tensioning it, and then I won't tighten it down til he has everything off. Traction is off, right? Now go ahead and put the traction back on.
There's our rim down. Okay, so it's not so floppy now. So it’s nice and stable there. Nice and firm there. That’s not going anywhere. Now this is normally lax. This is more medial. These are the areas here. If you're going to put another one, it would only be if this extended out laterally, which it didn't cuz there's my junction right there, see it? So I like that - I like that a lot. And everything is buried. When your head goes in, all this will be compressed, and then we’ll look at it from the peripheral compartment.
Now I’ll take the obturator for the blue. 70 on our pump. So we go 70 so we insufflate this joint to provide as much distention. That's our repair. Out the other side. Everything out that side - this side. So now we’re in the peripheral compartment. Look back, there's our labrum right there. That's your capsule reflection off the neck. Flex her up to about 40 - 45 degrees. And right there is your medial - medial plica in it. See it right there? If you get tumors, that’s where they like to hide out. So this is looking all the way medial right here.
So you can range her a little bit, and we're all the way medial, so we’ll start coming over lateral now. If we look up, this thing coming down is going to be your iliopsoas. So in between this medial synovial fold right here and her labrum right here is - straight up above is going to be her iliopsoas. This bulge I’m underneath, it’s a little bit frayed. I'm coming down there. And some people will have an exposure of the tendon with no capsule here. It’s pretty neat. You can look right up it. Look at a blood vessel right there. See a pulp.
So and this is my other reason for not doing T capsulorrhaphy - you cut across all this blood supply that's coming in through the capsule and that then goes into the labrum. If I cut across here, now that's not down here, but the main spot is right down here - right at the capsule labral junction is where the blood supply is, but you can see the huge feeders coming off that - look and look - you can see them going right into the labrum - look at it. See it? Yep. So why would you cut across that? It makes no sense to me - why you take a knife and cut that off. Yet to come up above it.
So there’s our medial synovial fold. We’ll come the other side here. Okay and this thing coming right here - this round thing - is the zona orbicularis. That's what the capsule ties into, and it allows that we can rotate this patient without the capsule getting tethered. It’s really truly in here. Here’s our suture, see it? See a suture? Great seal all the way around, you can follow it all the way around. Let's see, what are we up to? What number?